Das könnte Ihnen auch gefallen
- Immunological and Blood Products: Pharmaceutical MonographsVon EverandImmunological and Blood Products: Pharmaceutical MonographsNoch keine Bewertungen
- Nuevos Antibioticos Vs Gram NegativosDokument11 SeitenNuevos Antibioticos Vs Gram NegativosbrenpmNoch keine Bewertungen
- Jof 09 00171Dokument20 SeitenJof 09 00171Saman Kumara PereraNoch keine Bewertungen
- Drug Resistance TuberculosisDokument21 SeitenDrug Resistance TuberculosisfyonaxrkgredsxdwtNoch keine Bewertungen
- Microorganisms 09 02297 v2Dokument17 SeitenMicroorganisms 09 02297 v2yeayNoch keine Bewertungen
- Antibiotic Resistance of Bacteria: A Global Challenge: Saswati Sengupta and Madhab K ChattopadhyayDokument15 SeitenAntibiotic Resistance of Bacteria: A Global Challenge: Saswati Sengupta and Madhab K Chattopadhyaysourav dasNoch keine Bewertungen
- Ivermectin: A Systematic Review From Antiviral Effects To COVID-19 Complementary RegimenDokument10 SeitenIvermectin: A Systematic Review From Antiviral Effects To COVID-19 Complementary Regimenwn6ejrNoch keine Bewertungen
- Health Service Organisation Aaw 2021 Powerpoint PresentationDokument77 SeitenHealth Service Organisation Aaw 2021 Powerpoint Presentationhassan shahidNoch keine Bewertungen
- Antibiotics: Dr. Mushtak T. S. Al-OuqailiDokument107 SeitenAntibiotics: Dr. Mushtak T. S. Al-OuqailiSreenath Repakula100% (2)
- S Ynthesis, Characterization, Antitubercular and Antibacterial Activity, and Molecular Docking of 2,3-Disubstituted Quinazolinone Derivatives.Dokument12 SeitenS Ynthesis, Characterization, Antitubercular and Antibacterial Activity, and Molecular Docking of 2,3-Disubstituted Quinazolinone Derivatives.Rajasekhar KomarlaKumarachariNoch keine Bewertungen
- Antibiotic Use: Present and Future: Stephen H. ZinnerDokument5 SeitenAntibiotic Use: Present and Future: Stephen H. Zinnermbilouzi589Noch keine Bewertungen
- Mechanisms Efflux Pumps of Acinetobacter To Antibiotics: Baumannii (MDR) : Increasing ResistanceDokument23 SeitenMechanisms Efflux Pumps of Acinetobacter To Antibiotics: Baumannii (MDR) : Increasing ResistanceanggaririnNoch keine Bewertungen
- History of Antimicrobial Agents & Resistant BacteriaDokument6 SeitenHistory of Antimicrobial Agents & Resistant BacteriaAnurrag KumarNoch keine Bewertungen
- Perspectives: Where Will New Antibiotics Come From?Dokument6 SeitenPerspectives: Where Will New Antibiotics Come From?nabilahNoch keine Bewertungen
- Review On Cephalosporins Re ModifiedDokument6 SeitenReview On Cephalosporins Re Modifiedramirezgrisel966Noch keine Bewertungen
- CH631-unit-3 Med Chem PDFDokument77 SeitenCH631-unit-3 Med Chem PDFN Khadija BathoolNoch keine Bewertungen
- Veterinary Pharmacology and Therapeutics II Course OutlineDokument30 SeitenVeterinary Pharmacology and Therapeutics II Course OutlineAbdusaburNoch keine Bewertungen
- International Journal of Antimicrobial Agents: Ashish Yashwantrao PawarDokument3 SeitenInternational Journal of Antimicrobial Agents: Ashish Yashwantrao PawarPetroNoch keine Bewertungen
- Antibiotics Past, Present and Future 2019Dokument9 SeitenAntibiotics Past, Present and Future 2019Aylin GarcíaNoch keine Bewertungen
- Antibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)Dokument93 SeitenAntibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)francieudo1Noch keine Bewertungen
- International Journal of Pharma and Bio Sciences: Corresponding AuthorDokument6 SeitenInternational Journal of Pharma and Bio Sciences: Corresponding AuthoreditorofijtosNoch keine Bewertungen
- VPT 411: Veterinary Chemotherapy (2+0) : Syllabus TheoryDokument192 SeitenVPT 411: Veterinary Chemotherapy (2+0) : Syllabus TheoryDr Ashwini ShuklaNoch keine Bewertungen
- 2016 Oktober Kuliah Antimikroba TMD IntroductionDokument53 Seiten2016 Oktober Kuliah Antimikroba TMD IntroductionClara Shinta AruanNoch keine Bewertungen
- Safdar Et Al 2004 in Vivo Pharmacodynamic Activity of DaptomycinDokument6 SeitenSafdar Et Al 2004 in Vivo Pharmacodynamic Activity of DaptomycinduongnguyenNoch keine Bewertungen
- Multi Drug ResistanceDokument33 SeitenMulti Drug ResistanceEvanslin SantusNoch keine Bewertungen
- Antibacterial Efficacy of Metallic Nanoparticles of CaricaDokument12 SeitenAntibacterial Efficacy of Metallic Nanoparticles of CaricaTJPRC PublicationsNoch keine Bewertungen
- Antimycobacterial Activity of Quaternary Pyridinium Salts and Pyridinium N-OxidesDokument13 SeitenAntimycobacterial Activity of Quaternary Pyridinium Salts and Pyridinium N-OxidesSonguigama CoulibalyNoch keine Bewertungen
- Molecules: Antibacterial Prodrugs To Overcome Bacterial ResistanceDokument16 SeitenMolecules: Antibacterial Prodrugs To Overcome Bacterial Resistancealanbecker_alNoch keine Bewertungen
- 103 108 PDFDokument6 Seiten103 108 PDFMatiyas ZewdeNoch keine Bewertungen
- Atbs Cocos Pos MDRDokument24 SeitenAtbs Cocos Pos MDRvascoNoch keine Bewertungen
- Antibiotics 23101Dokument77 SeitenAntibiotics 23101TES SENNoch keine Bewertungen
- 747-Texto Del Artículo-2488-1-10-20200806Dokument2 Seiten747-Texto Del Artículo-2488-1-10-20200806Ruth BurgaNoch keine Bewertungen
- Antibiotic Resistance - A Global Issue of Concern: Rekha Bisht, Alok Katiyar, Rajat Singh, Piyush MittalDokument6 SeitenAntibiotic Resistance - A Global Issue of Concern: Rekha Bisht, Alok Katiyar, Rajat Singh, Piyush MittalBramaNoch keine Bewertungen
- Mekanisme Resistensi Antibiotik - 2014Dokument10 SeitenMekanisme Resistensi Antibiotik - 2014ArdieNoch keine Bewertungen
- Antibióticos, Quimioterápicos e Resistência MicrobianaDokument54 SeitenAntibióticos, Quimioterápicos e Resistência MicrobianaMarta BarbosaNoch keine Bewertungen
- 1 Antimicrobial ResistanceDokument27 Seiten1 Antimicrobial ResistanceLorenz L. Llamas IIINoch keine Bewertungen
- AntibioticsDokument22 SeitenAntibioticsSmiley QueenNoch keine Bewertungen
- 2 Acylamino 5 Nitro 1,3 Thiazoles PDFDokument8 Seiten2 Acylamino 5 Nitro 1,3 Thiazoles PDFJulianaRinconLopezNoch keine Bewertungen
- Chapter 9Dokument8 SeitenChapter 9Cagabcab Canibel MelanyNoch keine Bewertungen
- IUTTDokument19 SeitenIUTTWalid Ebid ElgammalNoch keine Bewertungen
- Potencial Uso de Ivermectina en Tratamiento y Profilaxis de Covid19Dokument18 SeitenPotencial Uso de Ivermectina en Tratamiento y Profilaxis de Covid19Andrimar Del Carmen Torres MuñozNoch keine Bewertungen
- Aslm 2018 Role of The Laboratory in AmrDokument37 SeitenAslm 2018 Role of The Laboratory in Amrphuong mai leNoch keine Bewertungen
- VPT 411 Veterinary Chemotherapy Tanuvas Lecture NotesDokument94 SeitenVPT 411 Veterinary Chemotherapy Tanuvas Lecture NotesSunil100% (41)
- The Use of Vancomycin With Its Therapeutic and Adverse Effects: A ReviewDokument11 SeitenThe Use of Vancomycin With Its Therapeutic and Adverse Effects: A Reviewdea yuniarNoch keine Bewertungen
- Antimicrobial Resistances: The World's Next Pandemic On The WayDokument11 SeitenAntimicrobial Resistances: The World's Next Pandemic On The WayIAEME PublicationNoch keine Bewertungen
- MICP LAB (WEEK - 5) Antimicrobial Agents in TherapydocDokument8 SeitenMICP LAB (WEEK - 5) Antimicrobial Agents in Therapydoccaitie miracleNoch keine Bewertungen
- Study Drug Resistance in Bacteria Using AntibioticsDokument47 SeitenStudy Drug Resistance in Bacteria Using Antibioticskioilui;lphio961% (18)
- Ofy 064Dokument3 SeitenOfy 064Robert StryjakNoch keine Bewertungen
- Hutchings 2019Dokument9 SeitenHutchings 2019nabilahNoch keine Bewertungen
- Potential Properties of Lactobacillus Plantarum F-10 As A Bio-Control Strategy For Wound InfectionsDokument14 SeitenPotential Properties of Lactobacillus Plantarum F-10 As A Bio-Control Strategy For Wound InfectionsIgor BaltaNoch keine Bewertungen
- Wound 2016 0701Dokument9 SeitenWound 2016 0701Ine Marthia DanieNoch keine Bewertungen
- Consensus On Wound Antisepsis - Update 2018Dokument31 SeitenConsensus On Wound Antisepsis - Update 2018Cuidados Enfermagem DomicílioNoch keine Bewertungen
- Ijms V6i8p103Dokument6 SeitenIjms V6i8p103Azzam SaqrNoch keine Bewertungen
- Colson 2016Dokument4 SeitenColson 2016rabbanibreNoch keine Bewertungen
- Possible Treatment and Strategies For COVID-19: Review and AssessmentDokument16 SeitenPossible Treatment and Strategies For COVID-19: Review and AssessmentAni RahayuNoch keine Bewertungen
- Post Test and CfuDokument13 SeitenPost Test and CfuMarie Fatima Quidet UdalbeNoch keine Bewertungen
- Antimicrobial Resistance in LeprosyDokument6 SeitenAntimicrobial Resistance in Leprosyintan rosliNoch keine Bewertungen
- Synthesis of New Thiazolide ProdrugsDokument23 SeitenSynthesis of New Thiazolide ProdrugsErick SalgadoNoch keine Bewertungen
- Antibiotics and FutureDokument16 SeitenAntibiotics and FutureSachithNoch keine Bewertungen
- Aula 5Dokument64 SeitenAula 5Mariana Barros Da Cruz AlunoNoch keine Bewertungen
- UG ENGLISH Honours PDFDokument59 SeitenUG ENGLISH Honours PDFMR.Shantanu SharmaNoch keine Bewertungen
- Operating Instructions: Rotary Lobe PumpDokument77 SeitenOperating Instructions: Rotary Lobe PumpRuslan SlusarNoch keine Bewertungen
- Joomag 2020 06 12 27485398153Dokument2 SeitenJoomag 2020 06 12 27485398153Vincent Deodath Bang'araNoch keine Bewertungen
- 2010 Information ExchangeDokument15 Seiten2010 Information ExchangeAnastasia RotareanuNoch keine Bewertungen
- HangersSupportsReferenceDataGuide PDFDokument57 SeitenHangersSupportsReferenceDataGuide PDFIndra RosadiNoch keine Bewertungen
- 5045.CHUYÊN ĐỀDokument8 Seiten5045.CHUYÊN ĐỀThanh HuyềnNoch keine Bewertungen
- Sociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadDokument44 SeitenSociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadJohn Blackburn100% (20)
- 01 - TechDocs, Acft Gen, ATAs-05to12,20 - E190 - 202pgDokument202 Seiten01 - TechDocs, Acft Gen, ATAs-05to12,20 - E190 - 202pgေအာင္ ရွင္း သန္ ့Noch keine Bewertungen
- Kortz Center GTA Wiki FandomDokument1 SeiteKortz Center GTA Wiki FandomsamNoch keine Bewertungen
- Investigation Data FormDokument1 SeiteInvestigation Data Formnildin danaNoch keine Bewertungen
- ABHA Coil ProportionsDokument5 SeitenABHA Coil ProportionsOctav OctavianNoch keine Bewertungen
- Springs: All India Distributer of NienhuisDokument35 SeitenSprings: All India Distributer of NienhuisIrina DroliaNoch keine Bewertungen
- Institutions and StrategyDokument28 SeitenInstitutions and StrategyFatin Fatin Atiqah100% (1)
- Makalah Bahasa Inggris TranslateDokument14 SeitenMakalah Bahasa Inggris TranslatevikaseptideyaniNoch keine Bewertungen
- JIMMA Electrical&ComputerEngDokument219 SeitenJIMMA Electrical&ComputerEngTewodros71% (7)
- 1Dokument2 Seiten1TrầnLanNoch keine Bewertungen
- Overlay Control PlansDokument1 SeiteOverlay Control PlansSTS-SPARK GAMINGNoch keine Bewertungen
- TechBridge TCP ServiceNow Business Case - Group 6Dokument9 SeitenTechBridge TCP ServiceNow Business Case - Group 6Takiyah Shealy100% (1)
- Learning Competency PDFDokument1 SeiteLearning Competency PDFLEOMAR PEUGALNoch keine Bewertungen
- B-GL-385-009 Short Range Anti-Armour Weapon (Medium)Dokument171 SeitenB-GL-385-009 Short Range Anti-Armour Weapon (Medium)Jared A. Lang100% (1)
- SCIENCE 11 WEEK 6c - Endogenic ProcessDokument57 SeitenSCIENCE 11 WEEK 6c - Endogenic ProcessChristine CayosaNoch keine Bewertungen
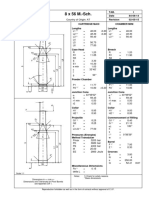
- 8 X 56 M.-SCH.: Country of Origin: ATDokument1 Seite8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNoch keine Bewertungen
- Capgemini - 2012-06-13 - 2012 Analyst Day - 3 - Michelin - A Better Way ForwardDokument12 SeitenCapgemini - 2012-06-13 - 2012 Analyst Day - 3 - Michelin - A Better Way ForwardAvanish VermaNoch keine Bewertungen
- You Can't Blame A FireDokument8 SeitenYou Can't Blame A FireMontana QuarterlyNoch keine Bewertungen
- Level of Organisation of Protein StructureDokument18 SeitenLevel of Organisation of Protein Structureyinghui94Noch keine Bewertungen
- BAMDokument111 SeitenBAMnageswara_mutyalaNoch keine Bewertungen
- Art Appreciation Chapter 3 SummaryDokument6 SeitenArt Appreciation Chapter 3 SummaryDiego A. Odchimar IIINoch keine Bewertungen
- Chapter 30 - HypertensionDokument70 SeitenChapter 30 - HypertensionSakaC.TanayaNoch keine Bewertungen
- Densha: Memories of A Train Ride Through Kyushu: By: Scott NesbittDokument7 SeitenDensha: Memories of A Train Ride Through Kyushu: By: Scott Nesbittapi-16144421Noch keine Bewertungen
- Collecting, Analyzing, & Feeding Back DiagnosticDokument12 SeitenCollecting, Analyzing, & Feeding Back DiagnosticCaroline Mariae TuquibNoch keine Bewertungen