Das könnte Ihnen auch gefallen
- Is It Real Can We Win Is It Worth DoingDokument32 SeitenIs It Real Can We Win Is It Worth DoingUsman FarooqNoch keine Bewertungen
- Patient Journey Mapping WorkshopDokument2 SeitenPatient Journey Mapping WorkshopPankaj MehrotraNoch keine Bewertungen
- Chest X Rays by ChristopherDokument1 SeiteChest X Rays by ChristopherAtulKaushikNoch keine Bewertungen
- Practice Marketing Plan FinalDokument14 SeitenPractice Marketing Plan Finalapi-317365152Noch keine Bewertungen
- Partners Case CCMNDokument4 SeitenPartners Case CCMNapi-314349758Noch keine Bewertungen
- Journey of PatientDokument77 SeitenJourney of PatientJaykishan MistryNoch keine Bewertungen
- MAPEH 10 TEST FOR THE FIRST GRADING PERIOD IN Grade 10 MAPEH (16-17)Dokument4 SeitenMAPEH 10 TEST FOR THE FIRST GRADING PERIOD IN Grade 10 MAPEH (16-17)RJLifeOfPedz100% (3)
- Staying Sharp Brain PuzzlesDokument18 SeitenStaying Sharp Brain PuzzlesAnurrag Kumar0% (1)
- 7 Household Items For Faster Fat LossDokument30 Seiten7 Household Items For Faster Fat LossLinda PrideNoch keine Bewertungen
- Perinatal Medicine: Clinical and Biochemical Aspects of the Evaluation, Diagnosis and Management of the Fetus and NewbornVon EverandPerinatal Medicine: Clinical and Biochemical Aspects of the Evaluation, Diagnosis and Management of the Fetus and NewbornNoch keine Bewertungen
- Branding & Positioning in HealthcareDokument86 SeitenBranding & Positioning in HealthcaresudhakerjadhavNoch keine Bewertungen
- Medical Center Marketing PlanDokument8 SeitenMedical Center Marketing PlanIan CastroNoch keine Bewertungen
- Ndometriosis: A Guide For PatientsDokument16 SeitenNdometriosis: A Guide For PatientsYusran AchmadNoch keine Bewertungen
- Deloitte Personalised Medicine Analysis-PGx-ROIDokument32 SeitenDeloitte Personalised Medicine Analysis-PGx-ROISimranjit SinghNoch keine Bewertungen
- Johnson & Johnson: "Caring For You From The Beginning, To The Very End!"Dokument18 SeitenJohnson & Johnson: "Caring For You From The Beginning, To The Very End!"Kaushik BalachandarNoch keine Bewertungen
- MS Obstetrics & Gynaecology - Plan of Thesis (Year 2015)Dokument4 SeitenMS Obstetrics & Gynaecology - Plan of Thesis (Year 2015)RachnaNoch keine Bewertungen
- Novartis NVS Q4 2016 Ir PresentationDokument84 SeitenNovartis NVS Q4 2016 Ir PresentationmedtechyNoch keine Bewertungen
- Cervical CancerDokument36 SeitenCervical CancerSatish ShresthaNoch keine Bewertungen
- PWC Pharma Success StrategiesDokument56 SeitenPWC Pharma Success StrategiesSanjay Gade100% (1)
- An Integrated Patient Journey Mapping Tool For Embedding Quality in Healthcare Service ReformDokument23 SeitenAn Integrated Patient Journey Mapping Tool For Embedding Quality in Healthcare Service Reformfatih jumongNoch keine Bewertungen
- Ethical Considerations of Fetal TherapyDokument13 SeitenEthical Considerations of Fetal TherapyRyan SadonoNoch keine Bewertungen
- Breaking Bad News (BHP)Dokument3 SeitenBreaking Bad News (BHP)nadiaayud100% (1)
- Primary Health Care As An Approach To HealthDokument31 SeitenPrimary Health Care As An Approach To HealthRea Andrea CuaresmaNoch keine Bewertungen
- Analysis of Preconception Healthcare Services Delivered in Selected Medical Officer of Health Areas of Kandy District in Sri LankaDokument10 SeitenAnalysis of Preconception Healthcare Services Delivered in Selected Medical Officer of Health Areas of Kandy District in Sri Lankachamil wijekoonNoch keine Bewertungen
- Rural Health Disparities: Public Health, Policy, and Planning ApproachesVon EverandRural Health Disparities: Public Health, Policy, and Planning ApproachesNoch keine Bewertungen
- Here Are 3 Benefits of Healthcare MarketingDokument3 SeitenHere Are 3 Benefits of Healthcare MarketingCIO Advisor ApacNoch keine Bewertungen
- Zuellig HXDokument5 SeitenZuellig HXAijem RyanNoch keine Bewertungen
- Building Patient LoyaltyDokument35 SeitenBuilding Patient LoyaltyFitri NihNoch keine Bewertungen
- 10 Ideas For Healthcare, 2012Dokument32 Seiten10 Ideas For Healthcare, 2012Roosevelt Campus NetworkNoch keine Bewertungen
- Oral Contraceptive PillsDokument113 SeitenOral Contraceptive PillsRaj KumarNoch keine Bewertungen
- Individual Project Updated VersionDokument2 SeitenIndividual Project Updated VersionsherifNoch keine Bewertungen
- Investing For Life: Meeting Poor People's Needs For Access To Medicines Through Responsible Business PracticesDokument57 SeitenInvesting For Life: Meeting Poor People's Needs For Access To Medicines Through Responsible Business PracticesOxfamNoch keine Bewertungen
- Why Every Doctor Needs A Personal BrandDokument3 SeitenWhy Every Doctor Needs A Personal BrandGirish JoshiNoch keine Bewertungen
- Hospital MarketinDokument47 SeitenHospital Marketinchandraprakash_shuklNoch keine Bewertungen
- WAO White Book On Allergy PDFDokument238 SeitenWAO White Book On Allergy PDFAura Lorena Rivas ZambranoNoch keine Bewertungen
- Advanced Certificate in Pharmacy: TH TH RDDokument8 SeitenAdvanced Certificate in Pharmacy: TH TH RDAhmed AnysNoch keine Bewertungen
- Using E-Technologies in Clinical Trials Rosa 2015Dokument14 SeitenUsing E-Technologies in Clinical Trials Rosa 2015Itzcoatl Torres AlcantaraNoch keine Bewertungen
- Recurrent Pregnancy LossDokument71 SeitenRecurrent Pregnancy LossshashankiswaitingNoch keine Bewertungen
- FNP 1 InfertilityDokument32 SeitenFNP 1 Infertilityapi-555392359Noch keine Bewertungen
- Road Map To PMTDokument2 SeitenRoad Map To PMTNarveer ShekhawatNoch keine Bewertungen
- Phosphorus Handout Word SearchDokument2 SeitenPhosphorus Handout Word Searchapi-239733253Noch keine Bewertungen
- Apollo Gleneagles HospitalsDokument23 SeitenApollo Gleneagles Hospitalssujal verma100% (1)
- Pricing Strategies in HealthcareDokument4 SeitenPricing Strategies in HealthcareAvantika ChaudharyNoch keine Bewertungen
- Global Pharma StrategyDokument15 SeitenGlobal Pharma StrategyDr Amit RangnekarNoch keine Bewertungen
- Gyn Screening PresentationDokument27 SeitenGyn Screening Presentationapi-437704700100% (1)
- Atorva Final PDFDokument19 SeitenAtorva Final PDFKshama ShahNoch keine Bewertungen
- User Research Questions For Dashboard DesignDokument3 SeitenUser Research Questions For Dashboard DesignAli AMNoch keine Bewertungen
- StartUp Health Insights 2020 Year-End ReportDokument13 SeitenStartUp Health Insights 2020 Year-End ReportLê Thanh HàNoch keine Bewertungen
- A Study On Marketing Strategy Used by Private Hospitals in GujaratDokument4 SeitenA Study On Marketing Strategy Used by Private Hospitals in GujaratInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Global Oncology Trends 2018 PDFDokument64 SeitenGlobal Oncology Trends 2018 PDFDr AKSHAY KANT CHATURVEDI100% (1)
- Investor Presentation Dec 2018 GeneralitatDokument35 SeitenInvestor Presentation Dec 2018 GeneralitatFernando HernandezNoch keine Bewertungen
- Kenya National Family Planning Guidelines 6th Edition-For PrintDokument216 SeitenKenya National Family Planning Guidelines 6th Edition-For PrintGrace MwangiNoch keine Bewertungen
- Current Health TechnologyDokument47 SeitenCurrent Health TechnologyDolisha WarbiNoch keine Bewertungen
- Call Planning Delivering On Brand StrategyDokument8 SeitenCall Planning Delivering On Brand StrategyjsarangocNoch keine Bewertungen
- Public Private Partnership in Health Care: Shiv Chandra MathurDokument14 SeitenPublic Private Partnership in Health Care: Shiv Chandra MathurUtpal DekaNoch keine Bewertungen
- Diabetes Mellitus in Pregnancy - Screening and DiagnosisDokument18 SeitenDiabetes Mellitus in Pregnancy - Screening and DiagnosisjjjkkNoch keine Bewertungen
- 10 Infectious DiseaseDokument42 Seiten10 Infectious Diseaseandirio7486Noch keine Bewertungen
- The New Normal For HealthDokument26 SeitenThe New Normal For Healthkyle gerome BayotNoch keine Bewertungen
- Class 1 Indian Medical Council ActDokument40 SeitenClass 1 Indian Medical Council ActJanet SweetyNoch keine Bewertungen
- Pregnancy PDFsDokument39 SeitenPregnancy PDFsOnPointRadioNoch keine Bewertungen
- The Investigation and Analysis of Critical Incidents and Adverse Events in HealthcareDokument162 SeitenThe Investigation and Analysis of Critical Incidents and Adverse Events in HealthcareBryan NguyenNoch keine Bewertungen
- Breastfeeding Manual Jan 31 2023Dokument43 SeitenBreastfeeding Manual Jan 31 2023Aqsa Munir100% (1)
- Gynecology Screening ProceduresDokument30 SeitenGynecology Screening Proceduresapi-506496190Noch keine Bewertungen
- Habitat For Humanity of Greater Stark & Carroll CountiesDokument12 SeitenHabitat For Humanity of Greater Stark & Carroll CountiesHan OWNoch keine Bewertungen
- Proposal Partners in HopeDokument16 SeitenProposal Partners in HopeHan OWNoch keine Bewertungen
- Proposal Community Preparatory SchoolDokument9 SeitenProposal Community Preparatory SchoolHan OWNoch keine Bewertungen
- Proven Study MethodsDokument8 SeitenProven Study MethodsHan OW100% (1)
- Ntravenous Fluids: How Much To GiveDokument1 SeiteNtravenous Fluids: How Much To GiveHan OWNoch keine Bewertungen
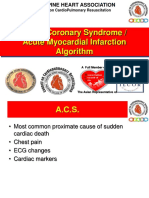
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDokument37 SeitenAcute Coronary Syndrome / Acute Myocardial Infarction AlgorithmHan OWNoch keine Bewertungen
- IV Drip Monitoring - ConceptDokument14 SeitenIV Drip Monitoring - ConceptHan OWNoch keine Bewertungen
- Social Determinants of HealthDokument42 SeitenSocial Determinants of HealthSharon DenhamNoch keine Bewertungen
- Toefl Ex 4Dokument3 SeitenToefl Ex 4Daniel MartínezNoch keine Bewertungen
- Fast Food RestaurantDokument19 SeitenFast Food RestaurantVivek GyawaliNoch keine Bewertungen
- Modeling Metabolic Adaptations and Energy Regulation in HumansDokument20 SeitenModeling Metabolic Adaptations and Energy Regulation in Humanssiranjeevi gurumaniNoch keine Bewertungen
- Candito Advanced Bench ProgramDokument11 SeitenCandito Advanced Bench ProgramRômulo Abreu VerçosaNoch keine Bewertungen
- EliteFTS ProgramsDokument83 SeitenEliteFTS ProgramsRyan Pan100% (1)
- Obesity in USADokument10 SeitenObesity in USASalman TahirNoch keine Bewertungen
- Amenorrhoea RemediesDokument8 SeitenAmenorrhoea RemediesHomeopathy TorrentsNoch keine Bewertungen
- Nurs FPX 4900 Assessment 1 Assessing The Problem Leadership Collaboration Communication Change Management and Policy ConsiderationsDokument5 SeitenNurs FPX 4900 Assessment 1 Assessing The Problem Leadership Collaboration Communication Change Management and Policy Considerationsjoohnsmith070Noch keine Bewertungen
- Reading 9Dokument2 SeitenReading 9Дар'я ЄгороваNoch keine Bewertungen
- FructoseDokument23 SeitenFructoseManish TiwariNoch keine Bewertungen
- Soal Bhs Inggris TH 2013 Try OutDokument12 SeitenSoal Bhs Inggris TH 2013 Try OutAdawiyah SetiawatiNoch keine Bewertungen
- Prevention of Heart DiseaseDokument43 SeitenPrevention of Heart DiseaseamitmokalNoch keine Bewertungen
- Keratinisation and CornificationDokument38 SeitenKeratinisation and Cornificationlizamjen100% (3)
- Robert Lustig-Tooth Decay and Liver Decay-The Nexus of Doctors and DentistsDokument154 SeitenRobert Lustig-Tooth Decay and Liver Decay-The Nexus of Doctors and DentistsEmine Alaaddinoglu100% (2)
- MIMS Doctor August 2015 RGDokument48 SeitenMIMS Doctor August 2015 RGDika MidbrainNoch keine Bewertungen
- tmpB8EB TMPDokument366 SeitentmpB8EB TMPFrontiersNoch keine Bewertungen
- Makalah Farmakoterapi ObesitasDokument10 SeitenMakalah Farmakoterapi ObesitasWahyunial JansiskaNoch keine Bewertungen
- Walking Facts and Figures 1: The Benefits of WalkingDokument6 SeitenWalking Facts and Figures 1: The Benefits of WalkingGilles MalatrayNoch keine Bewertungen
- ACE Inhibitors Vs ARBsDokument4 SeitenACE Inhibitors Vs ARBsRizqi Haqqum MNoch keine Bewertungen
- Comparison of Health-Related Quality of Life of Elderly With Hypertension Living in Long-Term Facility vs. CommunityDokument82 SeitenComparison of Health-Related Quality of Life of Elderly With Hypertension Living in Long-Term Facility vs. CommunityEllah ChristineNoch keine Bewertungen
- Common Med Surg Lab ValuesDokument5 SeitenCommon Med Surg Lab ValuesToMorrowNoch keine Bewertungen
- Final Notes PE2Dokument5 SeitenFinal Notes PE2israel seraficaNoch keine Bewertungen
- Hubungan Stres Dengan Kualitas Hidup Penderita Diabetes Mellitus Tipe 2Dokument9 SeitenHubungan Stres Dengan Kualitas Hidup Penderita Diabetes Mellitus Tipe 2Wirda RinaNoch keine Bewertungen
- Ys Sep 2015 EngDokument68 SeitenYs Sep 2015 EngAniket ShahNoch keine Bewertungen
- Components of Breast MilkDokument2 SeitenComponents of Breast MilkAlya Putri KhairaniNoch keine Bewertungen