Das könnte Ihnen auch gefallen
- Friedman VTE Bundle PDFDokument24 SeitenFriedman VTE Bundle PDFGerman Parra CNoch keine Bewertungen
- Module E Shock, MODS Roy Model-Oxygenation-Perfusion Required Readings (See Syllabus For Detailed Reading)Dokument7 SeitenModule E Shock, MODS Roy Model-Oxygenation-Perfusion Required Readings (See Syllabus For Detailed Reading)Jeff ZhouNoch keine Bewertungen
- MCP Guide BookDokument80 SeitenMCP Guide BookJeyakumar SNoch keine Bewertungen
- Hemorrhagic Disease of NewbornDokument13 SeitenHemorrhagic Disease of NewbornRabi Dhakal100% (1)
- Pregnancy and Labor at Fetal Malpresentations and Abnormal PelvisDokument40 SeitenPregnancy and Labor at Fetal Malpresentations and Abnormal PelvisCoral Srinivasa Ramalu100% (1)
- Journal Homepage: - : IntroductionDokument8 SeitenJournal Homepage: - : IntroductionIJAR JOURNALNoch keine Bewertungen
- Erythrobalstosis Fetalis - Bawa-AnDokument9 SeitenErythrobalstosis Fetalis - Bawa-AnyasiraNoch keine Bewertungen
- 9fetal Well Being in PregnancyDokument10 Seiten9fetal Well Being in PregnancyuouoNoch keine Bewertungen
- CRF in PregnancyDokument27 SeitenCRF in PregnancyJitendra AgrawalNoch keine Bewertungen
- Disease Condition:: Hyperemsis Gravidarum: DefinitionDokument4 SeitenDisease Condition:: Hyperemsis Gravidarum: DefinitionPriyanka JohnNoch keine Bewertungen
- Tmbool's Notes in Obstetrics and GynecologyDokument113 SeitenTmbool's Notes in Obstetrics and GynecologyFrom HumanNoch keine Bewertungen
- Case Study 29-APHDokument31 SeitenCase Study 29-APHZarul Naim Mohd TamiziNoch keine Bewertungen
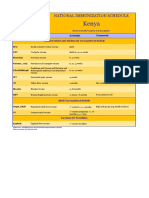
- Kenya Immunization ScheduleDokument1 SeiteKenya Immunization ScheduleDani AnyikaNoch keine Bewertungen
- Clinical Teaching 4PEUPERAL SEPSISDokument5 SeitenClinical Teaching 4PEUPERAL SEPSISAjit M Prasad PrasadNoch keine Bewertungen
- Hiv in PregnancyDokument98 SeitenHiv in PregnancyAkrit DahalNoch keine Bewertungen
- Pap Smear - Overview, Indications, PreparationDokument11 SeitenPap Smear - Overview, Indications, PreparationBayu Surya DanaNoch keine Bewertungen
- Chest Tube InsertionDokument4 SeitenChest Tube InsertionElton Dias PinheiroNoch keine Bewertungen
- Rhesus Isoimmunization: Ishen PerumalDokument29 SeitenRhesus Isoimmunization: Ishen PerumalIshen PerumalNoch keine Bewertungen
- Nature, Types, Causes and Methods of Abortion: ChapterDokument38 SeitenNature, Types, Causes and Methods of Abortion: ChapterBHUKYA USHARANINoch keine Bewertungen
- Trends in Midwifry and ObstetricsDokument8 SeitenTrends in Midwifry and ObstetricsVarna MohanNoch keine Bewertungen
- Instrumental and Distructive DeliveryDokument66 SeitenInstrumental and Distructive DeliveryDagnachew kasayeNoch keine Bewertungen
- Ministry of Health and Family Welfare Pregnancy GuidelinesDokument173 SeitenMinistry of Health and Family Welfare Pregnancy GuidelinesKhushi GuptaNoch keine Bewertungen
- International Journal of Trend in Scientific Research and Development (IJTSRD)Dokument16 SeitenInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNoch keine Bewertungen
- Management of Neonatal HypoglycemiaDokument14 SeitenManagement of Neonatal Hypoglycemiaece142Noch keine Bewertungen
- Normal Labour in Obstetric2Dokument17 SeitenNormal Labour in Obstetric2Tejasvi ChavdaNoch keine Bewertungen
- GyN OBS Updated MANAGEMENT PROTOCOL MOHDokument223 SeitenGyN OBS Updated MANAGEMENT PROTOCOL MOHyabsera mulatuNoch keine Bewertungen
- Hiv in Pregnant WomenDokument33 SeitenHiv in Pregnant WomenWill CheahNoch keine Bewertungen
- Extremely Low Birth Weight (ELBW) InfantDokument48 SeitenExtremely Low Birth Weight (ELBW) InfanthannanyusofNoch keine Bewertungen
- Antenatal ExaminationDokument18 SeitenAntenatal ExaminationMiu MiuNoch keine Bewertungen
- MusQan National Quality Assurance Standards and Assessment Tools For DH and CHCDokument274 SeitenMusQan National Quality Assurance Standards and Assessment Tools For DH and CHCRahul JalauniaNoch keine Bewertungen
- Or Report AmeerDokument16 SeitenOr Report AmeerYousef JafarNoch keine Bewertungen
- MalariaDokument42 SeitenMalariaNiraj Kumar100% (1)
- Labor and Delivery - 1Dokument32 SeitenLabor and Delivery - 1Lauren TrenchardNoch keine Bewertungen
- QP Code:111010 Reg. No: ........................ First Year B.SC Nursing Degree Examinations October 2017 Anatomy (2016 Scheme) Model Question PaperDokument6 SeitenQP Code:111010 Reg. No: ........................ First Year B.SC Nursing Degree Examinations October 2017 Anatomy (2016 Scheme) Model Question PaperdrsNoch keine Bewertungen
- 63 Shock in Obstetrics & GynecologyDokument29 Seiten63 Shock in Obstetrics & GynecologyGodsonYeboah-AwudziNoch keine Bewertungen
- BNSL 043 Block 4Dokument140 SeitenBNSL 043 Block 4Prabir Kumar Chatterjee100% (3)
- Gynecological Operation and Nursing ManagementDokument29 SeitenGynecological Operation and Nursing Managementhawra alsaadNoch keine Bewertungen
- The Abnormal PuerperiumDokument25 SeitenThe Abnormal PuerperiumMartijn JohanNoch keine Bewertungen
- 2017 STP Paed Neonates PDFDokument258 Seiten2017 STP Paed Neonates PDFChoden JamyangNoch keine Bewertungen
- ALLERGIC RHINITIS IN CHILDREN RinaDokument39 SeitenALLERGIC RHINITIS IN CHILDREN Rinarinajacky100% (2)
- Integrated Child Development Scheme (ICDS)Dokument30 SeitenIntegrated Child Development Scheme (ICDS)Geeta KumariNoch keine Bewertungen
- Oral Exam' Questions For V - Year Studying Students I Group of QuestionsDokument7 SeitenOral Exam' Questions For V - Year Studying Students I Group of QuestionsShreya SinghNoch keine Bewertungen
- Iv TherapyDokument3 SeitenIv TherapylovlyNoch keine Bewertungen
- Trail of LaborDokument5 SeitenTrail of LaborNithiya NadesanNoch keine Bewertungen
- Role of Midwifery NurseDokument6 SeitenRole of Midwifery NurseLokeshwari KatreNoch keine Bewertungen
- Oxytocics and TocolyticsDokument6 SeitenOxytocics and TocolyticsFarheen khanNoch keine Bewertungen
- Care of The Pregnant Woman With HIVDokument34 SeitenCare of The Pregnant Woman With HIVJenelle Melinda TullochNoch keine Bewertungen
- Multiple Pregnancies: Shanelle ThomasDokument40 SeitenMultiple Pregnancies: Shanelle Thomasshanellethomas1820100% (1)
- Hospital Management System SoftwareDokument11 SeitenHospital Management System SoftwareNikesh Solanki50% (2)
- E Lert OT LarmedDokument54 SeitenE Lert OT LarmedJetty Elizabeth JoseNoch keine Bewertungen
- Ethical Dilemmas in Picu: May Chehab, MD, FRCP (Lon), FRCP (Edin), ABIPDokument70 SeitenEthical Dilemmas in Picu: May Chehab, MD, FRCP (Lon), FRCP (Edin), ABIPmay chehabNoch keine Bewertungen
- Exclusive Breast Milk Nutrition For Baby 0-6 Month Only !Dokument4 SeitenExclusive Breast Milk Nutrition For Baby 0-6 Month Only !WindayaniayuNoch keine Bewertungen
- A Study To Assess The Knowledge of Postnatal Mothers Regarding Breast Engorgement in Nerkundrum IIDokument9 SeitenA Study To Assess The Knowledge of Postnatal Mothers Regarding Breast Engorgement in Nerkundrum IIEditor IJTSRDNoch keine Bewertungen
- AnthopometryDokument44 SeitenAnthopometryghifari2007Noch keine Bewertungen
- WHO Labour Care GuideDokument34 SeitenWHO Labour Care GuideAnkita Singh100% (1)
- OBG DrugsDokument85 SeitenOBG Drugsvivekkumar05468Noch keine Bewertungen
- INFERTILITY (AutoRecovered)Dokument13 SeitenINFERTILITY (AutoRecovered)Kafara EllisNoch keine Bewertungen
- Obstetric EmergenciesDokument28 SeitenObstetric EmergenciesRina Fatimah NurillahNoch keine Bewertungen
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesVon EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNoch keine Bewertungen
- Problem-based Approach to Gastroenterology and HepatologyVon EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNoch keine Bewertungen
- Suprapubic Prostatectomy HinmanDokument9 SeitenSuprapubic Prostatectomy HinmanputriNoch keine Bewertungen
- Hazardous Chemical Products in Home.Dokument17 SeitenHazardous Chemical Products in Home.taratarabuzuNoch keine Bewertungen
- Acog Embarazo Gemelar 2004 PDFDokument15 SeitenAcog Embarazo Gemelar 2004 PDFEliel MarcanoNoch keine Bewertungen
- Interpretation of Histograms and Its Correlation WDokument5 SeitenInterpretation of Histograms and Its Correlation WrezqiNoch keine Bewertungen
- MRCPass Notes For MRCP 1 - HEMATOLOGYDokument9 SeitenMRCPass Notes For MRCP 1 - HEMATOLOGYsabdali100% (1)
- Shaws Text Book of GynecologyDokument438 SeitenShaws Text Book of GynecologySumeera Nirmal Samarakkody100% (2)
- Home Private ServiceDokument4 SeitenHome Private ServiceTubagus Adil AL AminNoch keine Bewertungen
- Medicinal Plant (Rahul Sharma) ChambaDokument17 SeitenMedicinal Plant (Rahul Sharma) ChambaRahul SharmaNoch keine Bewertungen
- Emergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant ProfessorDokument45 SeitenEmergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant Professorpooja singhNoch keine Bewertungen
- Charkoli ProjectDokument2 SeitenCharkoli ProjectckbbbsrNoch keine Bewertungen
- Antifungal Susceptibility Pattern Against Dermatophytic Strains Isolated From Humans in Anambra State, NigeriaDokument8 SeitenAntifungal Susceptibility Pattern Against Dermatophytic Strains Isolated From Humans in Anambra State, NigeriaIJAERS JOURNALNoch keine Bewertungen
- Compatibility Between Space Analysis Methods of Kesling and Arch Length DiscrepancyDokument6 SeitenCompatibility Between Space Analysis Methods of Kesling and Arch Length DiscrepancynostaNoch keine Bewertungen
- Rab297cen - Yumizen H500 OT Daily Guide PDFDokument42 SeitenRab297cen - Yumizen H500 OT Daily Guide PDFZhafira Afsheen Niesa100% (2)
- Music Therapy Improves Sleep Quality in Acute and ChronicDokument12 SeitenMusic Therapy Improves Sleep Quality in Acute and ChronicLaras Ciingu SyahrezaNoch keine Bewertungen
- Tennis Elbow' or Lateral Epicondylitis: Information For YouDokument4 SeitenTennis Elbow' or Lateral Epicondylitis: Information For YouvivinNoch keine Bewertungen
- Tracheostomy CareDokument7 SeitenTracheostomy CareJoanna MayNoch keine Bewertungen
- Tinnitus EpidemiologyDokument149 SeitenTinnitus EpidemiologyTheodoros Kontogiannis100% (1)
- Inhibidores de La ECADokument16 SeitenInhibidores de La ECAFarmaFMNoch keine Bewertungen
- Blood Vessels and Circulation 1Dokument36 SeitenBlood Vessels and Circulation 1Kuya RnJNoch keine Bewertungen
- Orotol Plus GB 0118Dokument16 SeitenOrotol Plus GB 0118rahmatNoch keine Bewertungen
- Mary Oliver - US History Final ProjectDokument6 SeitenMary Oliver - US History Final ProjectMary OliverNoch keine Bewertungen
- Components of General Anesthesia: UnconsciousnessDokument17 SeitenComponents of General Anesthesia: UnconsciousnessDanieleNoch keine Bewertungen
- Aplicación de Un Programa de Entrenamiento de Fuerza en Futbolistas Jovenes PDFDokument16 SeitenAplicación de Un Programa de Entrenamiento de Fuerza en Futbolistas Jovenes PDFEsteban LopezNoch keine Bewertungen
- Observator Ios 2016Dokument355 SeitenObservator Ios 2016ajgamesNoch keine Bewertungen
- At The Doctor's: Speaker 1: I've Just Had AnDokument2 SeitenAt The Doctor's: Speaker 1: I've Just Had AnVictor0% (1)
- Ointment Box OutlineDokument1 SeiteOintment Box OutlineDon Nestor Razon Jr.Noch keine Bewertungen
- Paediatric Clerking SheetDokument5 SeitenPaediatric Clerking SheetIamTinesh100% (2)
- Bodytalk:: Exploring The 3 BrainsDokument31 SeitenBodytalk:: Exploring The 3 BrainsPenelopeReyesNoch keine Bewertungen
- Foundations Study Guide FINAL EXAMDokument15 SeitenFoundations Study Guide FINAL EXAMigorot89100% (1)
- Ground Floor PlanDokument1 SeiteGround Floor PlanjrsourisNoch keine Bewertungen