Das könnte Ihnen auch gefallen
- Referat Gangguan Lapang PandangDokument27 SeitenReferat Gangguan Lapang PandangIkrima MuhdarmuhallyNoch keine Bewertungen
- Tugas Baca RapdDokument76 SeitenTugas Baca RapdCecilia Casandra UneputtyNoch keine Bewertungen
- Laporan Kasus-Low Vision Dengan NystagmusDokument9 SeitenLaporan Kasus-Low Vision Dengan NystagmusDony Dwi PutraNoch keine Bewertungen
- Graves OphthalmopathyDokument27 SeitenGraves Ophthalmopathydevy100% (1)
- Retinopati HipertensiDokument14 SeitenRetinopati HipertensiFelais Hediyanto PradanaNoch keine Bewertungen
- Perbedaan Papila Dan Folikel Pada MataDokument2 SeitenPerbedaan Papila Dan Folikel Pada MataMuhammad Agus Nashir100% (1)
- Soal AAODokument33 SeitenSoal AAOwidyawirapNoch keine Bewertungen
- Diagnosis Banding KeratitisDokument7 SeitenDiagnosis Banding KeratitisNurwahidah Lakaming100% (2)
- Retina Examination and Drawing: CEH Retinal TeamDokument39 SeitenRetina Examination and Drawing: CEH Retinal TeamrzmNoch keine Bewertungen
- Trauma Dan Kegawatdaruratan MataDokument92 SeitenTrauma Dan Kegawatdaruratan MataM Isyhaduul IslamNoch keine Bewertungen
- Soal Subdivisi Roo Eyelid NeoplasmDokument8 SeitenSoal Subdivisi Roo Eyelid NeoplasmBudhi KaromaNoch keine Bewertungen
- Correlation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliDokument3 SeitenCorrelation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliKarina NathaniaNoch keine Bewertungen
- Corneal Drawing and Other StructureDokument2 SeitenCorneal Drawing and Other StructureOden Mahyudin50% (2)
- Referat Romzan Retinopathy of PrematurityDokument46 SeitenReferat Romzan Retinopathy of Prematurityromzanr97Noch keine Bewertungen
- Perbedaan Lesi Korteks Dan SubkortekDokument5 SeitenPerbedaan Lesi Korteks Dan SubkortekRisa SahiraNoch keine Bewertungen
- Laporan Kasus Os Posterior Vitreous Detachment (Floaters) : Pembimbing: Dr. Minggaringrum, SP.MDokument8 SeitenLaporan Kasus Os Posterior Vitreous Detachment (Floaters) : Pembimbing: Dr. Minggaringrum, SP.Malphonse yanuarNoch keine Bewertungen
- Laporan Kasus Katarak Fathonah (1102013108) .Id - enDokument48 SeitenLaporan Kasus Katarak Fathonah (1102013108) .Id - enAnonymous ZbhBxeEVNoch keine Bewertungen
- 386 Sindrom ParaneoplastikDokument3 Seiten386 Sindrom ParaneoplastikFathurrozi IdarNoch keine Bewertungen
- 14th SOM LAMPUNG 2020 PROPOSALDokument23 Seiten14th SOM LAMPUNG 2020 PROPOSALnovitaNoch keine Bewertungen
- Gambar UlkusDokument5 SeitenGambar UlkusMaria Margareta HutajuluNoch keine Bewertungen
- Corne A: Dr. Yulia Fitriani, SPMDokument47 SeitenCorne A: Dr. Yulia Fitriani, SPMEdsel QasswaraNoch keine Bewertungen
- 14 - 120218213815. Pneumonia Neonatal PDFDokument23 Seiten14 - 120218213815. Pneumonia Neonatal PDFOryza Malloen SativaNoch keine Bewertungen
- Workshop-Anamnesis & Pemeriksaan Oftalmologi Seminar IDIDokument57 SeitenWorkshop-Anamnesis & Pemeriksaan Oftalmologi Seminar IDIMichael FlynnNoch keine Bewertungen
- Diagnosis Banding Blok 23 Ulkus KorneaDokument16 SeitenDiagnosis Banding Blok 23 Ulkus KorneaAnggia Lestari HdyNoch keine Bewertungen
- Soal Refraksi AaoDokument4 SeitenSoal Refraksi Aaoria mutiaraNoch keine Bewertungen
- Abnormal Pupil, How To DoDokument8 SeitenAbnormal Pupil, How To DoUNHAS OphthalmologyNoch keine Bewertungen
- RGP Fitting +++++Dokument18 SeitenRGP Fitting +++++Philip McNelsonNoch keine Bewertungen
- Os Laserasi Palpebra Superior Full ThicknessDokument30 SeitenOs Laserasi Palpebra Superior Full ThicknessKemal TaufikNoch keine Bewertungen
- Lapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Dokument14 SeitenLapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Vincent RoorohNoch keine Bewertungen
- Soal Vignette NODokument5 SeitenSoal Vignette NOBima RizkiNoch keine Bewertungen
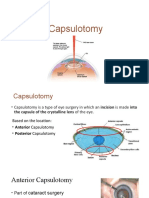
- CapsulotomyDokument15 SeitenCapsulotomyAdrian PearlNoch keine Bewertungen
- BronkiolitisDokument21 SeitenBronkiolitisRaditya Rangga PratamaNoch keine Bewertungen
- Reflex PupilDokument21 SeitenReflex PupilRaissaNoch keine Bewertungen
- Glaukoma Sudut Tertutup Primer Oculo Dextra SinistraDokument28 SeitenGlaukoma Sudut Tertutup Primer Oculo Dextra SinistraMariskaND100% (1)
- KeratitisDokument21 SeitenKeratitistifano_arian9684Noch keine Bewertungen
- RAPDDokument2 SeitenRAPDAlpascaFirdausNoch keine Bewertungen
- Papilledema Grading System (Frisen Scale)Dokument2 SeitenPapilledema Grading System (Frisen Scale)tesarNoch keine Bewertungen
- Hifema Slide (Autosaved)Dokument39 SeitenHifema Slide (Autosaved)febyolandaNoch keine Bewertungen
- DR Arief Priyadi SP.MDokument56 SeitenDR Arief Priyadi SP.MDarari GenaditaNoch keine Bewertungen
- Glaucoma GuidelinesDokument28 SeitenGlaucoma GuidelinesRina RostianaNoch keine Bewertungen
- Aao Bab 4Dokument3 SeitenAao Bab 4ria mutiaraNoch keine Bewertungen
- Subluksasi LensaDokument12 SeitenSubluksasi LensaDede GunawanNoch keine Bewertungen
- Humphrey Field AnalyzerTMDokument44 SeitenHumphrey Field AnalyzerTMsayumiholic890% (1)
- AniseikoniaDokument40 SeitenAniseikoniahenok biruk100% (1)
- Terjemahan Vaughan DDokument20 SeitenTerjemahan Vaughan DMelina Indah Sari100% (1)
- Nikolsky Sign and Koebner PhenomenonDokument8 SeitenNikolsky Sign and Koebner PhenomenonMuthia Khanza AbuBakarNoch keine Bewertungen
- Gangguan Involuntary MovementDokument54 SeitenGangguan Involuntary MovementMuammar RizkiNoch keine Bewertungen
- Oftalmologi Batch November 2017 - UnlockedDokument153 SeitenOftalmologi Batch November 2017 - Unlockeddzulkifli sukriNoch keine Bewertungen
- AmblyopiaDokument33 SeitenAmblyopiaSujon PaulNoch keine Bewertungen
- Board Januari 2009 Unair: GlaukomaDokument6 SeitenBoard Januari 2009 Unair: GlaukomaRizky AgustriaNoch keine Bewertungen
- Seidel's TestDokument13 SeitenSeidel's TestFahcrezaNoch keine Bewertungen
- Chapter 24 Preliminary Examination PDFDokument12 SeitenChapter 24 Preliminary Examination PDFfakenameNoch keine Bewertungen
- Materi KatarakDokument39 SeitenMateri KatarakfebyNoch keine Bewertungen
- Gonioscopy Technique and InterpretationDokument69 SeitenGonioscopy Technique and InterpretationAbegail IbañezNoch keine Bewertungen
- Introduction To Glaucoma': 1. Aqueous OutflowDokument17 SeitenIntroduction To Glaucoma': 1. Aqueous OutflowShari' Si WahyuNoch keine Bewertungen
- Gonioscopy1 PDFDokument74 SeitenGonioscopy1 PDFhestisuzetaNoch keine Bewertungen
- Open Angle GlaucomaDokument114 SeitenOpen Angle Glaucomahassan qureshiNoch keine Bewertungen
- GONIOSCOPY1Dokument74 SeitenGONIOSCOPY1partani_anand100% (1)
- ED Slit Lamp ExaminationDokument23 SeitenED Slit Lamp ExaminationNirmalie RupasingheNoch keine Bewertungen
- Anterior Chamber Angle Assessment TechniquesDokument29 SeitenAnterior Chamber Angle Assessment TechniquesSabyasachi100% (4)
- Research Article: TNF-Alpha Levels in Tears: A Novel Biomarker To Assess The Degree of Diabetic RetinopathyDokument7 SeitenResearch Article: TNF-Alpha Levels in Tears: A Novel Biomarker To Assess The Degree of Diabetic RetinopathytiaraleshaNoch keine Bewertungen
- 1 s2.0 S0886335018305959 Main PDFDokument7 Seiten1 s2.0 S0886335018305959 Main PDFtiaraleshaNoch keine Bewertungen
- Anesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFDokument11 SeitenAnesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFtiaraleshaNoch keine Bewertungen
- A Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosisDokument7 SeitenA Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosistiaraleshaNoch keine Bewertungen
- System. 3 Edition.: Daftar PustakaDokument2 SeitenSystem. 3 Edition.: Daftar PustakatiaraleshaNoch keine Bewertungen
- Dok Baru 2019-03-06 09.35.02 - 1Dokument1 SeiteDok Baru 2019-03-06 09.35.02 - 1tiaraleshaNoch keine Bewertungen
- Thala Semi ADokument41 SeitenThala Semi AtiaraleshaNoch keine Bewertungen
- The Perfect Answer Physics Revision Guide - Edexcel IGCSE 9-1 - 1st EditionDokument34 SeitenThe Perfect Answer Physics Revision Guide - Edexcel IGCSE 9-1 - 1st EditionKevir Man83% (6)
- Chapter 6 - Light and Optics (Student)Dokument25 SeitenChapter 6 - Light and Optics (Student)MAIMUNAH BINTI KHAIRUDDIN MoeNoch keine Bewertungen
- Optical Fiber Notes (Jan-2022)Dokument10 SeitenOptical Fiber Notes (Jan-2022)mandar desurkarNoch keine Bewertungen
- Transparent ConcreteDokument7 SeitenTransparent Concretekrishna reddyNoch keine Bewertungen
- Ray Optics and Optical InstrumentsDokument27 SeitenRay Optics and Optical InstrumentsSachin100% (1)
- SO OpticsDokument126 SeitenSO OpticsHollyNoch keine Bewertungen
- Optics: Properties of LightDokument52 SeitenOptics: Properties of LightSushmit GuptaNoch keine Bewertungen
- 2015 O-Level Physics Paper 2 Answer by Calvin Kong PhysicsDokument6 Seiten2015 O-Level Physics Paper 2 Answer by Calvin Kong PhysicsjesudassajNoch keine Bewertungen
- Ray Optics ModifyDokument178 SeitenRay Optics ModifyRaghuram SeshabhattarNoch keine Bewertungen
- Optical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andDokument19 SeitenOptical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andCarl SoriaNoch keine Bewertungen
- Answer With ExplanationDokument15 SeitenAnswer With ExplanationsenseiNoch keine Bewertungen
- Light - Reflection - Refraction - Diffraction - ReviewDokument42 SeitenLight - Reflection - Refraction - Diffraction - ReviewLester MarquezNoch keine Bewertungen
- Physics BookDokument50 SeitenPhysics Bookmadu1998Noch keine Bewertungen
- Electromagnetic WavesDokument23 SeitenElectromagnetic WavesNjike ChigbuNoch keine Bewertungen
- PhysicsDokument170 SeitenPhysicsW PremsonNoch keine Bewertungen
- MathsDokument23 SeitenMathsAstha UnadkatNoch keine Bewertungen
- QuestionsDokument16 SeitenQuestionsNowshin NamiraNoch keine Bewertungen
- Light Prism Pandathe Test2 Question PaperDokument4 SeitenLight Prism Pandathe Test2 Question Paperboltu100% (1)
- Short Answer Questions.: G M G M G M G MDokument6 SeitenShort Answer Questions.: G M G M G M G Mvishal_kalraNoch keine Bewertungen
- MATLAB Solution To Microwave Engineering Pozar 4th Ed. Example 1.5Dokument5 SeitenMATLAB Solution To Microwave Engineering Pozar 4th Ed. Example 1.5John Bofarull GuixNoch keine Bewertungen
- Total Internal ReflectionDokument17 SeitenTotal Internal Reflectionanand011Noch keine Bewertungen
- Bab 5 CahayaDokument11 SeitenBab 5 Cahayafazilarazali80Noch keine Bewertungen
- Chapter 33 Nature and Propagation of LightDokument63 SeitenChapter 33 Nature and Propagation of LightDilo TanNoch keine Bewertungen
- Optical Cables and Fibers V1.0-Excerption V2.0-201105-ADokument36 SeitenOptical Cables and Fibers V1.0-Excerption V2.0-201105-AKirandip SinghNoch keine Bewertungen
- WPhO (Singapore) - World Physics Olympiad (WPhO) - 2011Dokument20 SeitenWPhO (Singapore) - World Physics Olympiad (WPhO) - 2011GXGGXG50% (2)
- Physics Project On Tir Class 12Dokument17 SeitenPhysics Project On Tir Class 12fizakouser1216Noch keine Bewertungen
- EC 6702 Ocn Two MarksDokument24 SeitenEC 6702 Ocn Two MarksManiKandan SubbuNoch keine Bewertungen
- HCIP-Transmission V2.5 Training MaterialDokument840 SeitenHCIP-Transmission V2.5 Training MaterialEDWARD KIWALABYENoch keine Bewertungen
- Refraction DC DPPDokument1 SeiteRefraction DC DPParyanmcywaliaNoch keine Bewertungen
- Scientech 2502Dokument112 SeitenScientech 2502Abhay GargNoch keine Bewertungen