Das könnte Ihnen auch gefallen
- Yamada's Handbook of GastroenterologyVon EverandYamada's Handbook of GastroenterologyDr. Tadataka YamadaNoch keine Bewertungen
- INFERTILITYDokument48 SeitenINFERTILITYAyisha EdwinNoch keine Bewertungen
- InfertilityDokument14 SeitenInfertilityDrChauhanNoch keine Bewertungen
- English Ethical Issues in Obstetrics and GynecologyDokument148 SeitenEnglish Ethical Issues in Obstetrics and Gynecologyquinhox100% (1)
- APSA Fetal Handbook 2019Dokument92 SeitenAPSA Fetal Handbook 2019Fabrício GonzagaNoch keine Bewertungen
- Pediatric Surgery 2 (Respiratory and Gastrointestinal Conditions) PDFDokument12 SeitenPediatric Surgery 2 (Respiratory and Gastrointestinal Conditions) PDFRenatoCosmeGalvanJunior100% (1)
- Genito-Urinary Tract 37Dokument6 SeitenGenito-Urinary Tract 37Hasan A AsFourNoch keine Bewertungen
- SLEDokument42 SeitenSLETrishenth FonsekaNoch keine Bewertungen
- Management of Infertility: A Practical ApproachVon EverandManagement of Infertility: A Practical ApproachAntonio Simone LaganàNoch keine Bewertungen
- The Surgical Examination of ChildrenDokument315 SeitenThe Surgical Examination of ChildrenPatricia Beznea100% (1)
- GametogenesisDokument35 SeitenGametogenesisJason TulipatNoch keine Bewertungen
- Pediatric Surgery Handbook: June, 2013Dokument43 SeitenPediatric Surgery Handbook: June, 2013Azzam SaqrNoch keine Bewertungen
- Handbook of Pediatric Urology PDFDokument547 SeitenHandbook of Pediatric Urology PDFJany Bueno MontielNoch keine Bewertungen
- Imaging Diagnosis of Pancreatic Cancer: A State-Of-The-Art ReviewDokument15 SeitenImaging Diagnosis of Pancreatic Cancer: A State-Of-The-Art ReviewTanwirul JojoNoch keine Bewertungen
- Mainz II Surgery IllustratedDokument25 SeitenMainz II Surgery IllustratedPurvi ParikhNoch keine Bewertungen
- Pediatric Surgical Handbook PDFDokument139 SeitenPediatric Surgical Handbook PDFNia LahidaNoch keine Bewertungen
- Chapter Iv. Semen Analysis PDFDokument66 SeitenChapter Iv. Semen Analysis PDFCL Sanchez100% (1)
- Ifth DitionDokument25 SeitenIfth DitionAlfie Omega0% (1)
- Urinary IncontinenceDokument168 SeitenUrinary IncontinenceDumitritaNoch keine Bewertungen
- Pediatric Urology HDokument54 SeitenPediatric Urology HAlaa A. AbdelrahimNoch keine Bewertungen
- Images of Circumcision Complications Adult Circumcision Images Complications of Circumcision - Your Whole BabyDokument1 SeiteImages of Circumcision Complications Adult Circumcision Images Complications of Circumcision - Your Whole BabyPhoenixxx BeyNoch keine Bewertungen
- Infertility IDokument36 SeitenInfertility Idr_asaleh100% (1)
- Urinary IncontinenceDokument16 SeitenUrinary IncontinenceOana BalintNoch keine Bewertungen
- UROLOGYDokument222 SeitenUROLOGYBeso DavitashviliNoch keine Bewertungen
- Chapter 10 - Semen Analysis (Written Report) by Paglinawan, Et Al.Dokument9 SeitenChapter 10 - Semen Analysis (Written Report) by Paglinawan, Et Al.Martin Clyde100% (1)
- Anatomy of Male Organ of ReproductionDokument3 SeitenAnatomy of Male Organ of ReproductionrainbowrawrinshitNoch keine Bewertungen
- Anatomic Defects of The Abdominal WallDokument4 SeitenAnatomic Defects of The Abdominal WallKristen MontejoNoch keine Bewertungen
- Surgery Illustrated - Focus - Tapering of The MegaureterDokument5 SeitenSurgery Illustrated - Focus - Tapering of The MegauretermoetazNoch keine Bewertungen
- Benign Prostatic HypertrophyDokument111 SeitenBenign Prostatic HypertrophyOnkar SinghNoch keine Bewertungen
- Sacrococcygeal Teratoma - Paediatric Surgery UnitDokument74 SeitenSacrococcygeal Teratoma - Paediatric Surgery UnitOsasumwen OsagieNoch keine Bewertungen
- Help Pedsurgeryafricavolume01 PDFDokument413 SeitenHelp Pedsurgeryafricavolume01 PDFEbuwa AmadasunNoch keine Bewertungen
- Surgery Illustrated - Surgical Atlas: Mainz Pouch Continent Cutaneous DiversionDokument25 SeitenSurgery Illustrated - Surgical Atlas: Mainz Pouch Continent Cutaneous DiversionAbdullah Bangwar100% (1)
- 40 Phimosis 1Dokument8 Seiten40 Phimosis 1Navis Naldo AndreanNoch keine Bewertungen
- Laparoscopy: Shenillee Burgess Reyad HoseinDokument31 SeitenLaparoscopy: Shenillee Burgess Reyad HoseinShenillee BurgessNoch keine Bewertungen
- Urodynamics: Committee 7Dokument56 SeitenUrodynamics: Committee 7Coral Garcia RiveraNoch keine Bewertungen
- The Premature BabyDokument92 SeitenThe Premature BabyTrishenth Fonseka100% (1)
- Madanaman Diram Oct.142007 1-15Dokument15 SeitenMadanaman Diram Oct.142007 1-15Anshul Thakur100% (1)
- Clinical-Management STRATOG NEWDokument8 SeitenClinical-Management STRATOG NEWFarrukh Ali Khan100% (1)
- Manual of Laparoscopic UrologyDokument224 SeitenManual of Laparoscopic UrologyGeorge Delaca100% (1)
- Ureteric StentingVon EverandUreteric StentingRavi KulkarniNoch keine Bewertungen
- Post Liver Transplant ComplicationsDokument101 SeitenPost Liver Transplant ComplicationsWael Alkhiary100% (1)
- Pediatric Urology: Surgical Complications and ManagementVon EverandPediatric Urology: Surgical Complications and ManagementNoch keine Bewertungen
- Colorectal Oral Boards ReviewDokument79 SeitenColorectal Oral Boards Revieweztouch12Noch keine Bewertungen
- Undescended Testis, (Cryptorchidism) A Simple Guide To The Condition, Treatment And Related ConditionsVon EverandUndescended Testis, (Cryptorchidism) A Simple Guide To The Condition, Treatment And Related ConditionsBewertung: 5 von 5 Sternen5/5 (2)
- Antireflux Surgery Lich-GregoirDokument16 SeitenAntireflux Surgery Lich-GregoircristiangelsNoch keine Bewertungen
- Urology OralDokument2 SeitenUrology OralCorina TeteleaNoch keine Bewertungen
- Pediatric UrologyDokument80 SeitenPediatric UrologySav GaNoch keine Bewertungen
- Creog Urogyn ReviewDokument97 SeitenCreog Urogyn ReviewAlexandriah AlasNoch keine Bewertungen
- Sacrococcygeal Teratoma (SCT)Dokument5 SeitenSacrococcygeal Teratoma (SCT)IOSRjournalNoch keine Bewertungen
- 6 SURGERY II 6 - Pediatric UrologyDokument6 Seiten6 SURGERY II 6 - Pediatric UrologyDeann RoscomNoch keine Bewertungen
- 26.7.16-Approach To Ambiguous Genitalia - Is It A Boy or Girl PDFDokument57 Seiten26.7.16-Approach To Ambiguous Genitalia - Is It A Boy or Girl PDFBlueash BehNoch keine Bewertungen
- Copper Beaten Skull: Image QuizDokument3 SeitenCopper Beaten Skull: Image QuizLuwinda SariNoch keine Bewertungen
- 2010 GYN ModuleDokument36 Seiten2010 GYN Modulelolapell100% (1)
- Genital FistulaeDokument27 SeitenGenital Fistulaeapi-3705046100% (1)
- Fogsi ChecklistDokument131 SeitenFogsi ChecklistParimi VinodNoch keine Bewertungen
- Bunt - Male and Female Infertility USAFP 2009-v2 (PPTminimizer)Dokument35 SeitenBunt - Male and Female Infertility USAFP 2009-v2 (PPTminimizer)Jalajarani AridassNoch keine Bewertungen
- Pediatric Nephrology and Urology DR Samed AlsalmiDokument268 SeitenPediatric Nephrology and Urology DR Samed AlsalmitemisedwinNoch keine Bewertungen
- Snake Bite National Protocol PediatricsDokument45 SeitenSnake Bite National Protocol Pediatricsarjun_paulNoch keine Bewertungen
- Ob Gyn Soap NoteDokument1 SeiteOb Gyn Soap NoteMichelle Tanzil100% (1)
- The Gynecologic History and Pelvic Examination Up To Date 2016Dokument14 SeitenThe Gynecologic History and Pelvic Examination Up To Date 2016Mateo GlNoch keine Bewertungen
- Urology 90 Seconds - Buku 1Dokument202 SeitenUrology 90 Seconds - Buku 1Ari Alauddin100% (1)
- Total Pelvic ExenterationDokument13 SeitenTotal Pelvic ExenterationRirin Wahyuni100% (1)
- DR Shirin Surani Resident Year 1Dokument29 SeitenDR Shirin Surani Resident Year 1arjumandNoch keine Bewertungen
- Prostatitis AUA 2017Dokument29 SeitenProstatitis AUA 2017Andres Felipe Cordoba AriasNoch keine Bewertungen
- Complicated Labor and DeliveryDokument226 SeitenComplicated Labor and Deliveryrhimineecat71100% (1)
- 03 OSCE SlideShowDokument113 Seiten03 OSCE SlideShowMohamed FlefelNoch keine Bewertungen
- Quarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierDokument2 SeitenQuarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierTrishenth FonsekaNoch keine Bewertungen
- Quarterly Report On Case FindingDokument2 SeitenQuarterly Report On Case FindingTrishenth FonsekaNoch keine Bewertungen
- Quarterly Report On Program ManagementDokument7 SeitenQuarterly Report On Program ManagementTrishenth FonsekaNoch keine Bewertungen
- Quarterly Report On Microscopic Activities and LogisticsDokument2 SeitenQuarterly Report On Microscopic Activities and LogisticsTrishenth FonsekaNoch keine Bewertungen
- Quarterly Report On TB and non-TB WardsDokument3 SeitenQuarterly Report On TB and non-TB WardsTrishenth FonsekaNoch keine Bewertungen
- Quarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseDokument1 SeiteQuarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseTrishenth FonsekaNoch keine Bewertungen
- Duties of MOHDokument3 SeitenDuties of MOHTrishenth FonsekaNoch keine Bewertungen
- Laborotory Manual For Tuberculosis ControlDokument5 SeitenLaborotory Manual For Tuberculosis ControlTrishenth FonsekaNoch keine Bewertungen
- Register of TB SuspectsDokument1 SeiteRegister of TB SuspectsTrishenth FonsekaNoch keine Bewertungen
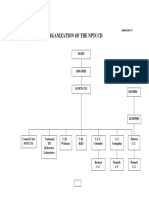
- Organization of NPTCCD PDFDokument2 SeitenOrganization of NPTCCD PDFTrishenth FonsekaNoch keine Bewertungen
- District TB RegisterDokument2 SeitenDistrict TB RegisterTrishenth FonsekaNoch keine Bewertungen
- 11 - Professional SecrecyDokument10 Seiten11 - Professional SecrecyTrishenth Fonseka100% (1)
- National TB Control ManualDokument223 SeitenNational TB Control ManualTrishenth FonsekaNoch keine Bewertungen
- Lab Form For Sputum Examination PDFDokument1 SeiteLab Form For Sputum Examination PDFTrishenth FonsekaNoch keine Bewertungen
- Gas Poisoning (Irrespirable Gases) : Asphyxial DeathDokument5 SeitenGas Poisoning (Irrespirable Gases) : Asphyxial DeathTrishenth FonsekaNoch keine Bewertungen
- QuotesDokument1 SeiteQuotesTrishenth FonsekaNoch keine Bewertungen
- Living With AFib Patient GuideDokument73 SeitenLiving With AFib Patient GuideTrishenth FonsekaNoch keine Bewertungen
- Neck Pain and Pain Down The ArmDokument27 SeitenNeck Pain and Pain Down The ArmTrishenth FonsekaNoch keine Bewertungen
- 13 - Medicolegal Duties of A DoctorDokument13 Seiten13 - Medicolegal Duties of A DoctorTrishenth FonsekaNoch keine Bewertungen
- 12 - Medical NegligenceDokument34 Seiten12 - Medical NegligenceTrishenth FonsekaNoch keine Bewertungen
- 15 - CN Poisoning 2Dokument2 Seiten15 - CN Poisoning 2Trishenth FonsekaNoch keine Bewertungen
- 29 - Heart Disease Complicating PregnancyDokument18 Seiten29 - Heart Disease Complicating PregnancyTrishenth FonsekaNoch keine Bewertungen
- 11 - SLMCDokument27 Seiten11 - SLMCTrishenth FonsekaNoch keine Bewertungen
- 11 - Medical EthicsDokument23 Seiten11 - Medical EthicsTrishenth FonsekaNoch keine Bewertungen
- 10 - Introduction To Legal System in SLDokument6 Seiten10 - Introduction To Legal System in SLTrishenth FonsekaNoch keine Bewertungen
- 08 - Post Mortem InstrumentsDokument6 Seiten08 - Post Mortem InstrumentsTrishenth FonsekaNoch keine Bewertungen
- 09 - Changes After Death and Time Since DeathDokument9 Seiten09 - Changes After Death and Time Since DeathTrishenth FonsekaNoch keine Bewertungen
- PhimosisDokument4 SeitenPhimosisHelvia Septarini TanjungNoch keine Bewertungen
- Lucija Kljaić Male Infertility: Course: Medical English 5Dokument11 SeitenLucija Kljaić Male Infertility: Course: Medical English 5Lucija KljaićNoch keine Bewertungen
- Reproduction in Human (Chapter 3) Teaching Notes - (Module 1)Dokument2 SeitenReproduction in Human (Chapter 3) Teaching Notes - (Module 1)succiniNoch keine Bewertungen
- SirkumsisiDokument15 SeitenSirkumsisirizal_lutfiNoch keine Bewertungen
- Daftar Alat-Alat Skill Lab: No Nama Alat No - Katalog - Merk Gambar Total Harga (RP) Qty Harga Satuan (RP)Dokument4 SeitenDaftar Alat-Alat Skill Lab: No Nama Alat No - Katalog - Merk Gambar Total Harga (RP) Qty Harga Satuan (RP)fk unramNoch keine Bewertungen
- Reproductive System of Sow BoarDokument32 SeitenReproductive System of Sow BoarMary Ann Derama ErginaNoch keine Bewertungen
- Spermatogenesis Is The Process by Which: Seminiferous Tubule With Maturing Sperm.Dokument2 SeitenSpermatogenesis Is The Process by Which: Seminiferous Tubule With Maturing Sperm.Garcia AzirNoch keine Bewertungen
- JURNAL IsnaDokument6 SeitenJURNAL IsnaRisnawati Abdul HarisNoch keine Bewertungen
- Phimosis 5 PDFDokument4 SeitenPhimosis 5 PDFNurul YaqinNoch keine Bewertungen
- Semen AnalysisDokument3 SeitenSemen AnalysisAnonymous tojT5nNoch keine Bewertungen
- Male Reproductive Anatomy - KWDokument26 SeitenMale Reproductive Anatomy - KWabyannaybaNoch keine Bewertungen
- Dr. Moch. Syahroni Far, Spu, M.KesDokument38 SeitenDr. Moch. Syahroni Far, Spu, M.KesNd EyeNoch keine Bewertungen
- 9 Male Reproductive System LectureDokument20 Seiten9 Male Reproductive System LectureGhadi RisNoch keine Bewertungen
- HPO FactSheet SexingKittensDokument1 SeiteHPO FactSheet SexingKittensKimNoch keine Bewertungen
- Reproductive SystemDokument7 SeitenReproductive Systemcollege code - 5Noch keine Bewertungen
- Sperm CountDokument2 SeitenSperm CountRamanasarmaNoch keine Bewertungen
- Semen Analysis and Preparation: Aysha ItaniDokument11 SeitenSemen Analysis and Preparation: Aysha ItaniFarid NurdiansyahNoch keine Bewertungen
- Male Reproductive SystemDokument44 SeitenMale Reproductive SystemTuaha MasoodNoch keine Bewertungen
- Undescended Testicles, Retractile Testicles, and Testicular TorsionDokument7 SeitenUndescended Testicles, Retractile Testicles, and Testicular TorsionYudhistira SuryamanggalaNoch keine Bewertungen
- Surgery Short Case - HydroceleDokument1 SeiteSurgery Short Case - HydroceleHeroNoch keine Bewertungen
- Elements of Morphology. Standard Terminology For External GenitaliaDokument26 SeitenElements of Morphology. Standard Terminology For External GenitaliaArturo RNoch keine Bewertungen
- Spermatocele in A South African Boerboel Dog: Andrea C. Hesser, DVM, Autumn P. Davidson, DVM, MS, Dipl. ACVIMDokument3 SeitenSpermatocele in A South African Boerboel Dog: Andrea C. Hesser, DVM, Autumn P. Davidson, DVM, MS, Dipl. ACVIMDNoch keine Bewertungen
- M12 Reproductive FertilityDokument6 SeitenM12 Reproductive Fertilityសេន វិចិត្ត Sen VichethNoch keine Bewertungen
- Yearling Bull Breeding Soundness ExaminationDokument14 SeitenYearling Bull Breeding Soundness ExaminationManu TabarezszNoch keine Bewertungen
- Evaluation of Extended Boar Semen After Glass Wool FiltrationDokument4 SeitenEvaluation of Extended Boar Semen After Glass Wool FiltrationRhyko DangkuNoch keine Bewertungen