Das könnte Ihnen auch gefallen
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionVon EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionNoch keine Bewertungen
- Pathology of Digestive SystemDokument28 SeitenPathology of Digestive SystemDianNursyifaRahmahNoch keine Bewertungen
- Selected Topics in the History of Biochemistry. Personal Recollections. Part IIIVon EverandSelected Topics in the History of Biochemistry. Personal Recollections. Part IIIBewertung: 1 von 5 Sternen1/5 (1)
- A Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table BelowDokument30 SeitenA Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table Belowinny100% (1)
- Thyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneDokument41 SeitenThyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneEsther AumaNoch keine Bewertungen
- Leishmania NewDokument27 SeitenLeishmania NewAnnu RajeshNoch keine Bewertungen
- Endocrine Disorders 1234399857677955 1Dokument130 SeitenEndocrine Disorders 1234399857677955 1api-19824701Noch keine Bewertungen
- Virus Host Interaction PDFDokument25 SeitenVirus Host Interaction PDFVEENA DEVINoch keine Bewertungen
- Rheumatoid Arthritis "An Autoimmune Mystery"Dokument23 SeitenRheumatoid Arthritis "An Autoimmune Mystery"Manisanthosh KumarNoch keine Bewertungen
- Precision Medicine NOTESDokument50 SeitenPrecision Medicine NOTESNishtha KhannaNoch keine Bewertungen
- Uworld GI NotesDokument17 SeitenUworld GI NotesAyodeji SotimehinNoch keine Bewertungen
- Salmonella: Praveen Rao, Sophia W. Riccardi, Danielle Birrer Seminar in Nucleic Acids-Spring 2004 Prof. ZubayDokument125 SeitenSalmonella: Praveen Rao, Sophia W. Riccardi, Danielle Birrer Seminar in Nucleic Acids-Spring 2004 Prof. ZubayPaolaForeroNoch keine Bewertungen
- BLOOD PHYSIOLOGY Study Notes For Medical StudentsDokument3 SeitenBLOOD PHYSIOLOGY Study Notes For Medical StudentsBijay Kumar MahatoNoch keine Bewertungen
- Innate & Adaptive Immunity (DR - Soraya Rezeki, MKT)Dokument30 SeitenInnate & Adaptive Immunity (DR - Soraya Rezeki, MKT)Dyah Wahlia100% (1)
- Inflammatory Bowel DiseaseDokument77 SeitenInflammatory Bowel DiseaseOmar mohamedNoch keine Bewertungen
- Glands of The Digestive SystemDokument16 SeitenGlands of The Digestive SystemMatija PajićNoch keine Bewertungen
- Hormon GDSDokument23 SeitenHormon GDSBRI KUNoch keine Bewertungen
- Exam3 BIOL1720 Fall2015Dokument5 SeitenExam3 BIOL1720 Fall2015NhiNoch keine Bewertungen
- Interpret Liver TestsDokument4 SeitenInterpret Liver TestsKaram Ali ShahNoch keine Bewertungen
- Base (Path Anatomy) 2014 FIRSTDokument39 SeitenBase (Path Anatomy) 2014 FIRSTHarsh NimavatNoch keine Bewertungen
- COPD Lecture Slides For BlackBoardDokument52 SeitenCOPD Lecture Slides For BlackBoardClayton JensenNoch keine Bewertungen
- Alzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoateDokument6 SeitenAlzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoatedineshhissarNoch keine Bewertungen
- 03 Cell InjuryDokument72 Seiten03 Cell InjuryLunaLure100% (1)
- AtaxiaDokument8 SeitenAtaxiaDivya Gupta0% (1)
- Liver DiseasesDokument335 SeitenLiver DiseasesdipakrussiaNoch keine Bewertungen
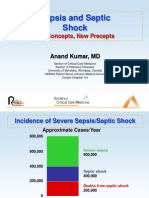
- Sepsis and Septic Shock: Old Concepts, New PreceptsDokument44 SeitenSepsis and Septic Shock: Old Concepts, New PreceptsEllagEszNoch keine Bewertungen
- Fatty Liver (1) - General PathologyDokument22 SeitenFatty Liver (1) - General PathologyDarien LiewNoch keine Bewertungen
- Group 2-Biochemistry-Pentose Pathway in A Relation To DiabetesDokument19 SeitenGroup 2-Biochemistry-Pentose Pathway in A Relation To DiabetesmonicachemsNoch keine Bewertungen
- GP Reg - Asthma and Spirometry 2011Dokument114 SeitenGP Reg - Asthma and Spirometry 2011minerva_stanciuNoch keine Bewertungen
- Ch11 - Cell Signaling SlidesDokument36 SeitenCh11 - Cell Signaling SlidesValine Cysteine MethionineNoch keine Bewertungen
- Amenorrhea WorkupDokument10 SeitenAmenorrhea WorkupHaoKeat HoeNoch keine Bewertungen
- Immunology NotesDokument8 SeitenImmunology NotesSumit Mukherjee100% (1)
- Autoimmunity PDFDokument73 SeitenAutoimmunity PDFErum JanNoch keine Bewertungen
- Poisoning II FinalDokument45 SeitenPoisoning II FinalBi PinNoch keine Bewertungen
- Fatty Liver and Cirrhosis - DR GurbilasDokument7 SeitenFatty Liver and Cirrhosis - DR GurbilasDr. Gurbilas P. SinghNoch keine Bewertungen
- Liver Tests SlidesDokument65 SeitenLiver Tests SlidesDokter MuhammadNoch keine Bewertungen
- HypertensionDokument85 SeitenHypertensionmelkamu AssefaNoch keine Bewertungen
- CataractsDokument24 SeitenCataractsMwamba ChikondeNoch keine Bewertungen
- UREMIADokument10 SeitenUREMIAAkanksha TiwariNoch keine Bewertungen
- Heat Shock ProteinsDokument98 SeitenHeat Shock ProteinsAprianie Wiwin100% (1)
- Elisa (Enzyme Linked Immunosorbant Assay)Dokument4 SeitenElisa (Enzyme Linked Immunosorbant Assay)Linette GuillermoNoch keine Bewertungen
- Freeze Etch MethodDokument3 SeitenFreeze Etch MethodNeha SinghalNoch keine Bewertungen
- Cough: PHR Sangita ShakyaDokument21 SeitenCough: PHR Sangita ShakyaCurex QANoch keine Bewertungen
- Cushing'S Syndrome: Roldan, Scorch Dominique Romero, John Reden Sanchez, Tracy JoyDokument25 SeitenCushing'S Syndrome: Roldan, Scorch Dominique Romero, John Reden Sanchez, Tracy JoyGerald John PazNoch keine Bewertungen
- Drowning: DR K.B.Suryakumar Prof & HOD Dept of Forensic Medicine KVG Medical College Sullia - KarnatakaDokument33 SeitenDrowning: DR K.B.Suryakumar Prof & HOD Dept of Forensic Medicine KVG Medical College Sullia - KarnatakaSuryakumar KilarNoch keine Bewertungen
- Nervous System Diseases and DisordersDokument88 SeitenNervous System Diseases and DisordersJape GarridoNoch keine Bewertungen
- Graves' Disease: Bella I. Putri 16-025Dokument29 SeitenGraves' Disease: Bella I. Putri 16-025anon_414347743Noch keine Bewertungen
- Fecal AnalysisDokument8 SeitenFecal AnalysisMafie BarreiroNoch keine Bewertungen
- Drug-Induced QT Interval ProlongationDokument13 SeitenDrug-Induced QT Interval ProlongationgeoaislaNoch keine Bewertungen
- Nature of DiseaseDokument14 SeitenNature of DiseaseLambo Ignacio Queen Quin100% (1)
- Inflammatory Bowel DiseaseDokument51 SeitenInflammatory Bowel DiseaseTeena Chandran100% (1)
- Acid-Base Disorders NotesDokument10 SeitenAcid-Base Disorders NotesLovely100% (1)
- Bacteriology Edited 1Dokument65 SeitenBacteriology Edited 1Ali AhmedNoch keine Bewertungen
- Arthritis, Infectious, BacterialDokument6 SeitenArthritis, Infectious, BacterialHarry IsraNoch keine Bewertungen
- Non Viral HepatitisDokument40 SeitenNon Viral Hepatitisostaz2000100% (1)
- Biochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDokument60 SeitenBiochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDr Kumar Ponnusamy100% (3)
- Candida and Other Fungi: Dr. John BergmanDokument60 SeitenCandida and Other Fungi: Dr. John Bergmanzeina32Noch keine Bewertungen
- Breast Pain - History TakingDokument6 SeitenBreast Pain - History TakingValencia FooNoch keine Bewertungen
- Obstructive UropathyDokument13 SeitenObstructive UropathyrizkyNoch keine Bewertungen
- The EarDokument68 SeitenThe EarSatyawira Aryawan Deng100% (1)
- Immunity - Blood ResponseDokument1 SeiteImmunity - Blood ResponseJustin Ahorro-DionisioNoch keine Bewertungen
- Ulcerative ColitisDokument1 SeiteUlcerative ColitisJustin Ahorro-DionisioNoch keine Bewertungen
- IRDS Sample Nursing ProblemsDokument5 SeitenIRDS Sample Nursing ProblemsJustin Ahorro-DionisioNoch keine Bewertungen
- IRDSDokument17 SeitenIRDSJustin Ahorro-DionisioNoch keine Bewertungen
- ImmunityDokument14 SeitenImmunityJustin Ahorro-DionisioNoch keine Bewertungen
- Patient's Bill of RightsDokument1 SeitePatient's Bill of RightsJustin Ahorro-DionisioNoch keine Bewertungen
- Endocrine DiseasesDokument170 SeitenEndocrine DiseasesJustin Ahorro-DionisioNoch keine Bewertungen
- GastrinomaDokument2 SeitenGastrinomaJustin Ahorro-DionisioNoch keine Bewertungen
- Immune Modulator: They Are Used To Modify The Actions of The Immune SystemDokument37 SeitenImmune Modulator: They Are Used To Modify The Actions of The Immune SystemJustin Ahorro-Dionisio100% (1)
- Fluid and ElectrolyteDokument57 SeitenFluid and ElectrolyteJustin Ahorro-DionisioNoch keine Bewertungen
- Fractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaDokument50 SeitenFractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaJustin Ahorro-DionisioNoch keine Bewertungen
- ColostomyDokument15 SeitenColostomyJustin Ahorro-DionisioNoch keine Bewertungen
- Gastro Intestinal SystemDokument48 SeitenGastro Intestinal SystemJustin Ahorro-DionisioNoch keine Bewertungen
- Factors Influencing AssessmentDokument2 SeitenFactors Influencing AssessmentJustin Ahorro-DionisioNoch keine Bewertungen
- Case Presentation: Ablay-Andrade-Batario-Berbano-Bibera-Borja-Borres-Burns - Cabañero-Corsiga-Custodio - CuyegkengDokument122 SeitenCase Presentation: Ablay-Andrade-Batario-Berbano-Bibera-Borja-Borres-Burns - Cabañero-Corsiga-Custodio - CuyegkengJustin Ahorro-Dionisio67% (3)
- Ego Defense MechanismDokument9 SeitenEgo Defense MechanismJustin Ahorro-DionisioNoch keine Bewertungen
- Embolic StrokeDokument2 SeitenEmbolic StrokeJustin Ahorro-DionisioNoch keine Bewertungen
- Couvade Syndrome and PseudocyesisDokument4 SeitenCouvade Syndrome and PseudocyesisJustin Ahorro-DionisioNoch keine Bewertungen
- Coxa PlanaDokument1 SeiteCoxa PlanaHazel EndayaNoch keine Bewertungen
- Coxa PlanaDokument13 SeitenCoxa PlanaJustin Ahorro-DionisioNoch keine Bewertungen
- COPD PathophysiologyDokument1 SeiteCOPD PathophysiologyJustin Ahorro-Dionisio33% (3)
- Conflict Management: Sources of Conflict Types of Conflict Conflict ResolutionDokument14 SeitenConflict Management: Sources of Conflict Types of Conflict Conflict ResolutionJustin Ahorro-Dionisio100% (1)
- Common Apparatus and ProceduresDokument7 SeitenCommon Apparatus and ProceduresNorazrina Abdul Aziz0% (1)
- Presentation of DiptheriaDokument45 SeitenPresentation of DiptheriaR-o-N-n-e-lNoch keine Bewertungen
- Coronary Artery DiseaseDokument7 SeitenCoronary Artery DiseaseJustin Ahorro-DionisioNoch keine Bewertungen
- Fluid and Electrolyte ImbalancesDokument21 SeitenFluid and Electrolyte Imbalanceschardel_08Noch keine Bewertungen
- Colostomy and The GallbladderDokument13 SeitenColostomy and The GallbladderJustin Ahorro-DionisioNoch keine Bewertungen
- Cardiovascular System5Dokument77 SeitenCardiovascular System5Justin Ahorro-DionisioNoch keine Bewertungen
- Chronic Lymphocytic LeukemiaDokument20 SeitenChronic Lymphocytic LeukemiaJustin Ahorro-Dionisio100% (1)
- FNCP'sDokument35 SeitenFNCP'scathypolidoNoch keine Bewertungen
- DWDMDokument41 SeitenDWDMKarthik KompelliNoch keine Bewertungen
- Smarajit Ghosh - Control Systems - Theory and Applications-Pearson (2006) PDFDokument629 SeitenSmarajit Ghosh - Control Systems - Theory and Applications-Pearson (2006) PDFaggarwalakanksha100% (2)
- Glossario - GETTY - IngDokument24 SeitenGlossario - GETTY - IngFabio ZarattiniNoch keine Bewertungen
- Applied Social Research A Tool For The Human Services 9th Edition Monette Test Bank 1Dokument36 SeitenApplied Social Research A Tool For The Human Services 9th Edition Monette Test Bank 1wesleyvasquezmeoapcjtrb100% (25)
- 039-Itp For Embedded Plate PDFDokument7 Seiten039-Itp For Embedded Plate PDFKöksal PatanNoch keine Bewertungen
- Module No.3 Prepare Architectual Job Requirements Architectural Working DrawingDokument23 SeitenModule No.3 Prepare Architectual Job Requirements Architectural Working DrawingJay S. On100% (1)
- Repro Indo China Conf PDFDokument16 SeitenRepro Indo China Conf PDFPavit KaurNoch keine Bewertungen
- Finite Element Method For Eigenvalue Problems in ElectromagneticsDokument38 SeitenFinite Element Method For Eigenvalue Problems in ElectromagneticsBhargav BikkaniNoch keine Bewertungen
- CP AssignmentDokument5 SeitenCP AssignmentMSSM EngineeringNoch keine Bewertungen
- FloodDokument9 SeitenFloodapi-352767278Noch keine Bewertungen
- CFA L1 Ethics Questions and AnswersDokument94 SeitenCFA L1 Ethics Questions and AnswersMaulik PatelNoch keine Bewertungen
- 11-Potential Use of Volcanic Pumice As A Construction Materialhossain2004Dokument7 Seiten11-Potential Use of Volcanic Pumice As A Construction Materialhossain2004afzal taiNoch keine Bewertungen
- Preparation of Kevlar-49 Fabric/E-Glass Fabric/Epoxy Composite Materials and Characterization of Their Mechanical PropertiesDokument10 SeitenPreparation of Kevlar-49 Fabric/E-Glass Fabric/Epoxy Composite Materials and Characterization of Their Mechanical PropertiesIndhu ElangoNoch keine Bewertungen
- BTL Marketing CompanyDokument30 SeitenBTL Marketing Companypradip_kumarNoch keine Bewertungen
- Defence QuestionnaireDokument2 SeitenDefence QuestionnaireSumitt SinghNoch keine Bewertungen
- Analysis of Mozarts k.475Dokument2 SeitenAnalysis of Mozarts k.475ASPASIA FRAGKOUNoch keine Bewertungen
- HOWO SERVICE AND MAINTENANCE SCHEDULE SinotruckDokument3 SeitenHOWO SERVICE AND MAINTENANCE SCHEDULE SinotruckRPaivaNoch keine Bewertungen
- Antibiotic I and II HWDokument4 SeitenAntibiotic I and II HWAsma AhmedNoch keine Bewertungen
- Urban LifestyleDokument27 SeitenUrban LifestyleNindy AslindaNoch keine Bewertungen
- T-61.246 Digital Signal Processing and Filtering T-61.246 Digitaalinen Signaalink Asittely Ja Suodatus Description of Example ProblemsDokument35 SeitenT-61.246 Digital Signal Processing and Filtering T-61.246 Digitaalinen Signaalink Asittely Ja Suodatus Description of Example ProblemsDoğukan TuranNoch keine Bewertungen
- Grammar and Oral Language Development (GOLD) : Reported By: Melyn A. Bacolcol Kate Batac Julie Ann OcampoDokument17 SeitenGrammar and Oral Language Development (GOLD) : Reported By: Melyn A. Bacolcol Kate Batac Julie Ann Ocampoclara dupitasNoch keine Bewertungen
- Plant Gardening AerationDokument4 SeitenPlant Gardening Aerationut.testbox7243Noch keine Bewertungen
- I. Level of Barriers in ICT Knowledge, Skills, and Competencies No ICT Knowledge, Skills and Competency Barriers SDA DA N A SADokument2 SeitenI. Level of Barriers in ICT Knowledge, Skills, and Competencies No ICT Knowledge, Skills and Competency Barriers SDA DA N A SAMuhamad KhoerulNoch keine Bewertungen
- OD - SAP Connector UtilityDokument22 SeitenOD - SAP Connector UtilityShivani SharmaNoch keine Bewertungen
- Fallas Compresor Copeland-DesbloqueadoDokument16 SeitenFallas Compresor Copeland-DesbloqueadoMabo MabotecnicaNoch keine Bewertungen
- MPH EocDokument8 SeitenMPH EocGalaleldin AliNoch keine Bewertungen
- PhysioEx Exercise 1 Activity 1Dokument3 SeitenPhysioEx Exercise 1 Activity 1edvin merida proNoch keine Bewertungen
- Control Flow, Arrays - DocDokument34 SeitenControl Flow, Arrays - DocHARIBABU N SEC 2020Noch keine Bewertungen
- Veris Case StudyDokument2 SeitenVeris Case StudyPankaj GargNoch keine Bewertungen
- Check Out The Buyers Guide On FacebookDokument28 SeitenCheck Out The Buyers Guide On FacebookCoolerAdsNoch keine Bewertungen
- Peaceful Sleep Hypnosis: Meditate & RelaxVon EverandPeaceful Sleep Hypnosis: Meditate & RelaxBewertung: 4.5 von 5 Sternen4.5/5 (142)
- Breaking the Habit of Being YourselfVon EverandBreaking the Habit of Being YourselfBewertung: 4.5 von 5 Sternen4.5/5 (1458)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissVon EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissBewertung: 4.5 von 5 Sternen4.5/5 (81)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipVon EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipBewertung: 4.5 von 5 Sternen4.5/5 (1135)
- Gut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Von EverandGut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Bewertung: 4.5 von 5 Sternen4.5/5 (20)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningVon EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningBewertung: 4 von 5 Sternen4/5 (3)
- Love Yourself, Heal Your Life Workbook (Insight Guide)Von EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Bewertung: 5 von 5 Sternen5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Bedtime Stories for Adults: Tales to Soothe the Tired SoulsVon EverandBedtime Stories for Adults: Tales to Soothe the Tired SoulsBewertung: 4 von 5 Sternen4/5 (3)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerVon EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerBewertung: 4.5 von 5 Sternen4.5/5 (58)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- Really Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityVon EverandReally Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityBewertung: 5 von 5 Sternen5/5 (28)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonVon EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonBewertung: 3.5 von 5 Sternen3.5/5 (33)
- Deep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellVon EverandDeep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellBewertung: 5 von 5 Sternen5/5 (8)
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Von EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Bewertung: 4.5 von 5 Sternen4.5/5 (10)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayVon EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNoch keine Bewertungen
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeVon EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeBewertung: 3.5 von 5 Sternen3.5/5 (13)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingVon EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingBewertung: 4.5 von 5 Sternen4.5/5 (103)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouVon EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouBewertung: 3.5 von 5 Sternen3.5/5 (5)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookVon EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingVon EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingBewertung: 4 von 5 Sternen4/5 (3)
- Fast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperVon EverandFast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperBewertung: 4.5 von 5 Sternen4.5/5 (15)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyVon EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNoch keine Bewertungen