Das könnte Ihnen auch gefallen
- IV Therapy EssentialsDokument57 SeitenIV Therapy Essentialsrye08Noch keine Bewertungen
- Introduction To Nursing PharmacologyDokument6 SeitenIntroduction To Nursing PharmacologyArun Roa DanielNoch keine Bewertungen
- 2nd Lecture Normal Phsiological Changes of Aging Final1.Ppt40-41Dokument85 Seiten2nd Lecture Normal Phsiological Changes of Aging Final1.Ppt40-41halayehiahNoch keine Bewertungen
- Focus Charting in Pedia WardDokument32 SeitenFocus Charting in Pedia Ward2A - Nicole Marrie HonradoNoch keine Bewertungen
- Nursing Skills ChecklistDokument6 SeitenNursing Skills Checklistapi-433700464Noch keine Bewertungen
- Copd Case StudyDokument6 SeitenCopd Case StudyDivine ParagasNoch keine Bewertungen
- MastitisDokument5 SeitenMastitisAnonymous Kv0sHqFNoch keine Bewertungen
- Atenolol TenorminDokument3 SeitenAtenolol TenorminLIEZEL GRACE VELAYONoch keine Bewertungen
- GROUP 3 - CASE STUDY - TraumaDokument5 SeitenGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculNoch keine Bewertungen
- Urinary CatheterizationDokument2 SeitenUrinary CatheterizationFains YdbwidNoch keine Bewertungen
- TLG IV TherapyDokument10 SeitenTLG IV TherapyStephanie Joy EscalaNoch keine Bewertungen
- NANDA DX NI, NODokument165 SeitenNANDA DX NI, NOKerry Brown100% (1)
- Eye GelDokument4 SeitenEye GelAjax YadavNoch keine Bewertungen
- Anatomy Dr. Aguirre Pancreas: ND RDDokument3 SeitenAnatomy Dr. Aguirre Pancreas: ND RDAlbert CorderoNoch keine Bewertungen
- Chapter 14 Intravenous Solutions, Equipment, and CalculationsDokument48 SeitenChapter 14 Intravenous Solutions, Equipment, and CalculationsEn Ras100% (1)
- IV Fluid Administration PG 2-15Dokument6 SeitenIV Fluid Administration PG 2-15secondtexanNoch keine Bewertungen
- InfluenzaDokument2 SeitenInfluenzajohnndoeeNoch keine Bewertungen
- Cardiac Testing Role Risk Stratifying ED Chest PainDokument17 SeitenCardiac Testing Role Risk Stratifying ED Chest PainGiorgiana pNoch keine Bewertungen
- Shock Concept MapDokument2 SeitenShock Concept MapElizabeth GarretsonNoch keine Bewertungen
- Muscle Strength TestingDokument3 SeitenMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- 7-Nervous SystemDokument69 Seiten7-Nervous SystemCarl Vincent VingnoNoch keine Bewertungen
- Case Study Thyroid NADokument10 SeitenCase Study Thyroid NARenae HueningNoch keine Bewertungen
- Back CareDokument20 SeitenBack Caresafina khstoonNoch keine Bewertungen
- Client Consultation Form - Pedicure AppoinmentDokument3 SeitenClient Consultation Form - Pedicure AppoinmentMicheal McDowellNoch keine Bewertungen
- Module 4 - Nebulization Through Aerosol Mask Metered-Dose Inhaler STUDENTDokument5 SeitenModule 4 - Nebulization Through Aerosol Mask Metered-Dose Inhaler STUDENTfebie pachecoNoch keine Bewertungen
- Nursing Care During Labor and Pain Management2015Dokument51 SeitenNursing Care During Labor and Pain Management2015christopher ebarbNoch keine Bewertungen
- Nursing Care Plans For Diabetes MellitusDokument12 SeitenNursing Care Plans For Diabetes MellitusPuteri AzmanNoch keine Bewertungen
- NCLEX Questions: Nursing Care, Medication Administration & Client EducationDokument3 SeitenNCLEX Questions: Nursing Care, Medication Administration & Client EducationkxviperNoch keine Bewertungen
- DSM-IV Schizophrenia Types and AssessmentDokument32 SeitenDSM-IV Schizophrenia Types and AssessmentJoyVee Pillagara-De LeonNoch keine Bewertungen
- IV Insertion ProcedureDokument11 SeitenIV Insertion ProcedureEdelweiss Marie Cayetano100% (1)
- Newborn Hearing Screening GuidelinesDokument2 SeitenNewborn Hearing Screening GuidelinesAileen A. MonaresNoch keine Bewertungen
- Vaccination or ImmunizationDokument4 SeitenVaccination or ImmunizationPrincessNoch keine Bewertungen
- OxygenationDokument12 SeitenOxygenationCherry Lou Guanzing100% (1)
- Immediate Newborn Care Updates at San Isidro CollegeDokument11 SeitenImmediate Newborn Care Updates at San Isidro CollegeMay Princes Torregosa Abucejo100% (1)
- Longifene ... Longifene-... Stimulone: Available BrandsDokument2 SeitenLongifene ... Longifene-... Stimulone: Available BrandsJustin Raul Dela CuadraNoch keine Bewertungen
- Classification of Burns Based On Depth CharacteristicsDokument2 SeitenClassification of Burns Based On Depth CharacteristicsmexelleNoch keine Bewertungen
- Homeostasis Temperature RegulationDokument22 SeitenHomeostasis Temperature RegulationChris AllamNoch keine Bewertungen
- Burns Rule of Nines 2013Dokument1 SeiteBurns Rule of Nines 2013ellenningrumNoch keine Bewertungen
- Unit 8: Pain Assessment and ManagementDokument24 SeitenUnit 8: Pain Assessment and ManagementMatthew RyanNoch keine Bewertungen
- Drugs Used in TuberculosisDokument27 SeitenDrugs Used in Tuberculosisapi-3705123Noch keine Bewertungen
- Geriatric OPD and Grand Rounds JournalDokument2 SeitenGeriatric OPD and Grand Rounds JournalOrlea Francisco-SisioNoch keine Bewertungen
- Advanced Infection Prevention and PDFDokument28 SeitenAdvanced Infection Prevention and PDFWardah Fauziah El SofwanNoch keine Bewertungen
- ABG Specimen Collection GuideDokument7 SeitenABG Specimen Collection GuideVangie OriginesNoch keine Bewertungen
- Types of Insulin PDFDokument3 SeitenTypes of Insulin PDFRetno WulanNoch keine Bewertungen
- Tracheostomy CareDokument7 SeitenTracheostomy CareICNREVILONoch keine Bewertungen
- Client Intake Form - NailsDokument2 SeitenClient Intake Form - NailsGGenZ ConsultingNoch keine Bewertungen
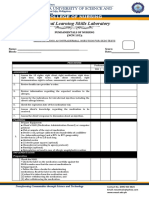
- Clinical Learning Skills Laboratory: College of NursingDokument3 SeitenClinical Learning Skills Laboratory: College of NursingBeverly DatuNoch keine Bewertungen
- Linezolid: Antibiotic ClassDokument2 SeitenLinezolid: Antibiotic ClassEdison Patricio Vallejo PasquelNoch keine Bewertungen
- TCL Immunization UPDATEDDokument43 SeitenTCL Immunization UPDATEDlaarnieNoch keine Bewertungen
- Burns MGNT and CalculationDokument7 SeitenBurns MGNT and CalculationPoova RagavanNoch keine Bewertungen
- IV Medication Check-ListDokument7 SeitenIV Medication Check-Listhewmour androidNoch keine Bewertungen
- Health Teaching Plan Age 76Dokument2 SeitenHealth Teaching Plan Age 76Mandy Martin100% (1)
- Hips Back Ankles Buttocks HeelsDokument13 SeitenHips Back Ankles Buttocks Heelsفرزدق الحسيناويNoch keine Bewertungen
- Fluanxol Depot: Name of MedicineDokument11 SeitenFluanxol Depot: Name of MedicineIvo_NichtNoch keine Bewertungen
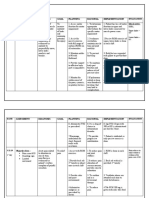
- Nursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataDokument8 SeitenNursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataMoonNoch keine Bewertungen
- Lesson 5 - Oxygen TherapyDokument16 SeitenLesson 5 - Oxygen TherapyDewi PrasetiaNoch keine Bewertungen
- MastitisDokument35 SeitenMastitisRestu AWNoch keine Bewertungen
- Types of Drug Preparation (Credit To The Rightful Owner)Dokument1 SeiteTypes of Drug Preparation (Credit To The Rightful Owner)Keren Grace EspirituNoch keine Bewertungen
- HNN215 Drug Diary GuideDokument10 SeitenHNN215 Drug Diary GuideMaddison MitchellNoch keine Bewertungen
- Emergency Cardiac Medications for ArrhythmiasDokument14 SeitenEmergency Cardiac Medications for ArrhythmiasRomzy BasañesNoch keine Bewertungen
- Classification Des MedicamentsDokument28 SeitenClassification Des MedicamentsTewfik TGr100% (1)
- Pharmacology - A Summary of Common ConditionsDokument50 SeitenPharmacology - A Summary of Common ConditionsJeremy YangNoch keine Bewertungen
- Antiarrhythmic AgentsDokument45 SeitenAntiarrhythmic AgentsSoh Kae SiangNoch keine Bewertungen
- PVC Unido ConDuplicadosDokument1.181 SeitenPVC Unido ConDuplicadosJorge Chachaima MarNoch keine Bewertungen
- Medication CardsDokument65 SeitenMedication CardsMovaliya Ghanshyam80% (5)
- Drug Interaction MonitoringDokument5 SeitenDrug Interaction MonitoringAnonymousNoch keine Bewertungen
- Icu DrugsDokument205 SeitenIcu DrugsAli50% (2)
- Resuscitation: ILCOR Summary StatementDokument13 SeitenResuscitation: ILCOR Summary StatementLuis-alfredo Perez Bolde HernandezNoch keine Bewertungen
- Toxicology CasesDokument65 SeitenToxicology CasesLalo LandaNoch keine Bewertungen
- 1 QE Competency 1 Therapeutic MOCK Test 1 QA May 2013Dokument54 Seiten1 QE Competency 1 Therapeutic MOCK Test 1 QA May 2013Yathrika YathrikaNoch keine Bewertungen
- Pearls of MRCP Part 2 PastestDokument111 SeitenPearls of MRCP Part 2 PastestS TNoch keine Bewertungen
- Pepsci RecallDokument3 SeitenPepsci RecallRumana AliNoch keine Bewertungen
- PeriarestDokument5 SeitenPeriarestMustafa ŠabićNoch keine Bewertungen
- Adverse Drug ReactionDokument53 SeitenAdverse Drug ReactionShruthi ReddyNoch keine Bewertungen
- Special Resource: Drugs To Be Used With A Filter For Preparation And/or AdministrationDokument5 SeitenSpecial Resource: Drugs To Be Used With A Filter For Preparation And/or Administrationemiliow_1Noch keine Bewertungen
- Kartu Kode ObatDokument2 SeitenKartu Kode ObatHerdaru DyahNoch keine Bewertungen
- Dược Động Học SlideDokument24 SeitenDược Động Học SlideDược NamNoch keine Bewertungen
- Pharmacology Mock Exam MCQDokument8 SeitenPharmacology Mock Exam MCQanaeshklNoch keine Bewertungen
- Drugs Used in CcuDokument169 SeitenDrugs Used in CcuAnusha Verghese100% (3)
- Emergency Drugs KathDokument29 SeitenEmergency Drugs Kathmajin655Noch keine Bewertungen
- Pharmacology Whole Imp PointsDokument23 SeitenPharmacology Whole Imp PointsSHAKEEL1991Noch keine Bewertungen
- Atrial Fibrillation GuideDokument7 SeitenAtrial Fibrillation GuideFirstglobalsupercopNoch keine Bewertungen
- E - Cart DrugsDokument18 SeitenE - Cart Drugs'SheenMarkReal'100% (2)
- ACLS PharmacologyDokument5 SeitenACLS PharmacologyKuruva MallikarjunaNoch keine Bewertungen
- Drug CalculationDokument34 SeitenDrug CalculationMalathi VarnaNoch keine Bewertungen
- Drugs Used in The Treatment of ArrhythmiasDokument37 SeitenDrugs Used in The Treatment of ArrhythmiasChipego ChiyaamaNoch keine Bewertungen
- MRCP Part 1-Pharm GuestionsDokument42 SeitenMRCP Part 1-Pharm GuestionswyenyNoch keine Bewertungen
- Updatesincardiacarrest Resuscitation: Vivian Lam,, Cindy H. HsuDokument15 SeitenUpdatesincardiacarrest Resuscitation: Vivian Lam,, Cindy H. HsuFia Bella KusumaNoch keine Bewertungen
- Haemoptysis Diagnosis and TreatmentDokument57 SeitenHaemoptysis Diagnosis and TreatmentMuhammad Cholid AlfahroziNoch keine Bewertungen