Das könnte Ihnen auch gefallen
- Myeloproliferative Disorders: UST. Tamer Imad UMST, Head of HaematologyDokument19 SeitenMyeloproliferative Disorders: UST. Tamer Imad UMST, Head of HaematologyNaiem MohammedNoch keine Bewertungen
- Schilling TestDokument10 SeitenSchilling TestNaiem MohammedNoch keine Bewertungen
- Myelodysplastic Syndromes (MDS) : Ust - Tamer Imad Head of Haematology Dept. MLS, UMSTDokument8 SeitenMyelodysplastic Syndromes (MDS) : Ust - Tamer Imad Head of Haematology Dept. MLS, UMSTNaiem MohammedNoch keine Bewertungen
- Schilling TestDokument10 SeitenSchilling TestNaiem MohammedNoch keine Bewertungen
- Sampling Fixation in CytologyDokument31 SeitenSampling Fixation in CytologyNaiem MohammedNoch keine Bewertungen
- Theory of Normal HaemostasisDokument18 SeitenTheory of Normal HaemostasisNaiem MohammedNoch keine Bewertungen
- The RHB Lood Gro Ups Yste M: Ust - Tam Er Im AdDokument19 SeitenThe RHB Lood Gro Ups Yste M: Ust - Tam Er Im AdNaiem MohammedNoch keine Bewertungen
- Multiple Myeloma: Ust - Tamer Imad Head of Haematology Dept. MLS, UMSTDokument5 SeitenMultiple Myeloma: Ust - Tamer Imad Head of Haematology Dept. MLS, UMSTNaiem MohammedNoch keine Bewertungen
- Primary Haemostatic Abnormalitis: MR - Tamer Imad Haematology DepartmentDokument15 SeitenPrimary Haemostatic Abnormalitis: MR - Tamer Imad Haematology DepartmentNaiem MohammedNoch keine Bewertungen
- Immunehaematology: UST. Tamer Imad UMST, Haematology DepartmentDokument38 SeitenImmunehaematology: UST. Tamer Imad UMST, Haematology DepartmentNaiem MohammedNoch keine Bewertungen
- Pap Smear ProcedureDokument14 SeitenPap Smear ProcedureNaiem MohammedNoch keine Bewertungen
- Diff-Quick Staining For CytologyDokument8 SeitenDiff-Quick Staining For CytologyNaiem MohammedNoch keine Bewertungen
- 9-Urine CytologyDokument14 Seiten9-Urine CytologyNaiem MohammedNoch keine Bewertungen
- 9-Urine CytologyDokument14 Seiten9-Urine CytologyNaiem MohammedNoch keine Bewertungen
- Sampling Fixation in CytologyDokument31 SeitenSampling Fixation in CytologyNaiem MohammedNoch keine Bewertungen
- Seminal Fluid: M. M. Al MakiDokument14 SeitenSeminal Fluid: M. M. Al MakiNaiem MohammedNoch keine Bewertungen
- ColestridiumDokument43 SeitenColestridiumNaiem MohammedNoch keine Bewertungen
- Sterilization14Dokument18 SeitenSterilization14Naiem MohammedNoch keine Bewertungen
- Specimen CollectionDokument24 SeitenSpecimen CollectionNaiem MohammedNoch keine Bewertungen
- Oxidase Test Tetramethyl Paraphenylene Diamine DihydrochlorideDokument10 SeitenOxidase Test Tetramethyl Paraphenylene Diamine DihydrochlorideNaiem MohammedNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- COPC V9 Final PDFDokument2 SeitenCOPC V9 Final PDFMohd Ismail YusofNoch keine Bewertungen
- Chevron Ursa SuperPlus EC 15w40 271201 MSDSDokument7 SeitenChevron Ursa SuperPlus EC 15w40 271201 MSDSImam Saja DechNoch keine Bewertungen
- Anther Pollen CultureDokument28 SeitenAnther Pollen CultureSachin MauryaNoch keine Bewertungen
- Practical 1: Determination of Reducing Sugar Using The Dinitrosalicylic (DNS) Colourimetric MethodDokument8 SeitenPractical 1: Determination of Reducing Sugar Using The Dinitrosalicylic (DNS) Colourimetric MethodNurSyazaHaniNoch keine Bewertungen
- Iran Syria AllianceDokument45 SeitenIran Syria AllianceOlga LazinNoch keine Bewertungen
- Cultural Web NHS StrategyDokument4 SeitenCultural Web NHS StrategyÄßħīłăşħ ĹăĐĐüNoch keine Bewertungen
- Genetics Case Study - MicrocephalyDokument4 SeitenGenetics Case Study - MicrocephalyHeru WNoch keine Bewertungen
- Other Requirement: BA-0496 Refap1 Project Disengager / Stripper R-300002, R-300003Dokument7 SeitenOther Requirement: BA-0496 Refap1 Project Disengager / Stripper R-300002, R-300003GLEDSONNoch keine Bewertungen
- Hamstring Flexibility GuideDokument14 SeitenHamstring Flexibility GuideHubert Selormey100% (4)
- VK Newsletter April 2016 - March 2017Dokument27 SeitenVK Newsletter April 2016 - March 2017HMIS VKBORLNoch keine Bewertungen
- Checklist Boeing 777Dokument5 SeitenChecklist Boeing 777Jacopo TediosiNoch keine Bewertungen
- Constant Voltage Constant Current DC Power SupplyDokument56 SeitenConstant Voltage Constant Current DC Power SupplySeven HillsNoch keine Bewertungen
- CE 132 - Geotechnical Engineering 2Dokument38 SeitenCE 132 - Geotechnical Engineering 2hahaduNoch keine Bewertungen
- Vol. 2 - Module 4 Act. - APPEARANCEDokument41 SeitenVol. 2 - Module 4 Act. - APPEARANCEryan binalayNoch keine Bewertungen
- ELK-3 420C 1HC0086882ABEnDokument20 SeitenELK-3 420C 1HC0086882ABEnMOHAMMED ALINoch keine Bewertungen
- Excel Containment SizingDokument7 SeitenExcel Containment SizingAbraham JyothimonNoch keine Bewertungen
- Cisplatin Monograph 1jul2016Dokument11 SeitenCisplatin Monograph 1jul2016Kurnia AnharNoch keine Bewertungen
- Is 7322Dokument16 SeitenIs 7322Vignesh NadimuthuNoch keine Bewertungen
- Extra homework-Che-XDokument3 SeitenExtra homework-Che-XBornil Bikash BhuyanNoch keine Bewertungen
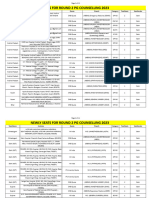
- Newly Seats For Round 2 PG Counselling 2023Dokument11 SeitenNewly Seats For Round 2 PG Counselling 2023Manoj KumarNoch keine Bewertungen
- Is Brain Death Actually DeathDokument20 SeitenIs Brain Death Actually DeathMário RibeiroNoch keine Bewertungen
- Transformer Protection ReviewDokument21 SeitenTransformer Protection ReviewcalecaleNoch keine Bewertungen
- DPI Report On WCPSS IDEA ComplianceDokument10 SeitenDPI Report On WCPSS IDEA ComplianceKeung HuiNoch keine Bewertungen
- HPWJ Safety Procedures RIL ARCDokument17 SeitenHPWJ Safety Procedures RIL ARCvishal bailurNoch keine Bewertungen
- About Nestle IndiaDokument5 SeitenAbout Nestle IndiaSAMBHAVI SINGH 1827653Noch keine Bewertungen
- Module 1 - Lecture 2Dokument32 SeitenModule 1 - Lecture 2Bruce bannerNoch keine Bewertungen
- HX400D6R AFJE3E 355CC-125 400-3-50 DatasheetDokument1 SeiteHX400D6R AFJE3E 355CC-125 400-3-50 DatasheetNduP78Noch keine Bewertungen
- Sponsorship Form 2022Dokument2 SeitenSponsorship Form 2022api-556012725Noch keine Bewertungen
- P1 Quality Management SystemDokument21 SeitenP1 Quality Management SystemShahadat HossainNoch keine Bewertungen
- LLENAS - DLL Sci 9 - Sept 5 9 KMLDokument6 SeitenLLENAS - DLL Sci 9 - Sept 5 9 KMLNicole Eve Pelaez-AbarrientosNoch keine Bewertungen