Das könnte Ihnen auch gefallen
- Malnutrition in the ElderlyVon EverandMalnutrition in the ElderlyW.O. SeilerNoch keine Bewertungen
- Nutrition Essentials The Secrets of Food and Body for Healthy LifeVon EverandNutrition Essentials The Secrets of Food and Body for Healthy LifeNoch keine Bewertungen
- Protein Energy Malnutrition (PEM)Dokument55 SeitenProtein Energy Malnutrition (PEM)AnuNoch keine Bewertungen
- Lec.6 Malnutrition in ChildrenDokument18 SeitenLec.6 Malnutrition in Childrenبركان معتصم مطشرNoch keine Bewertungen
- Disease PEMDokument16 SeitenDisease PEMMeena KoushalNoch keine Bewertungen
- Nutritional AssessmentDokument56 SeitenNutritional AssessmentJuvana LachuNoch keine Bewertungen
- PemDokument57 SeitenPemحمزةياسرحبيبNoch keine Bewertungen
- Marasmus KwashiorkorDokument49 SeitenMarasmus Kwashiorkorinoenk santosoNoch keine Bewertungen
- 1 NCM 116Dokument378 Seiten1 NCM 116Alkiana SalardaNoch keine Bewertungen
- Protein Energy Malnutrition Among Chil DrenDokument34 SeitenProtein Energy Malnutrition Among Chil DrenJay RathvaNoch keine Bewertungen
- (ND2) MalnutritionDokument18 Seiten(ND2) Malnutritionpdsth7mtsjNoch keine Bewertungen
- Nutrition: Malnutrition by DR Farhana Jabeen ShahDokument133 SeitenNutrition: Malnutrition by DR Farhana Jabeen ShahKamran Ahmad KhanNoch keine Bewertungen
- Assignment: ON Role of Community Health Nurse in Management of Malnourished ChildDokument48 SeitenAssignment: ON Role of Community Health Nurse in Management of Malnourished ChildSuman MondalNoch keine Bewertungen
- Malnutrition in Children For PDR III - PediaDokument24 SeitenMalnutrition in Children For PDR III - PediaJaniel King100% (1)
- Common Health Problems of NutritionDokument39 SeitenCommon Health Problems of NutritionShereen Mohamed Soliman HammoudaNoch keine Bewertungen
- NCM 116Dokument78 SeitenNCM 1166pk4c7kw4kNoch keine Bewertungen
- Nutritional Problems: Presenter Priyanka Gehlot M. Sc. (Prev.)Dokument38 SeitenNutritional Problems: Presenter Priyanka Gehlot M. Sc. (Prev.)vikas takNoch keine Bewertungen
- UndernutritionDokument37 SeitenUndernutritionRetno Mandriyarini67% (3)
- Nutrition ProblemsDokument11 SeitenNutrition Problemsvikas tak100% (2)
- Malnutrition DisordersDokument47 SeitenMalnutrition DisordersAnnisa AstariNoch keine Bewertungen
- Nutritional Disorders 1Dokument55 SeitenNutritional Disorders 1nukenNoch keine Bewertungen
- University of Mysore Government Home Science College HassanDokument23 SeitenUniversity of Mysore Government Home Science College HassanGaurav SindhiyaNoch keine Bewertungen
- Unit - I Introduction: Subjects Notes BSC Nursing Part - I Subject: NutritionDokument14 SeitenUnit - I Introduction: Subjects Notes BSC Nursing Part - I Subject: NutritionHemant SharmaNoch keine Bewertungen
- KwashiorkorDokument4 SeitenKwashiorkorDanti NurdindayantiNoch keine Bewertungen
- MALNUTRITIONDokument20 SeitenMALNUTRITIONJaphter MoongaNoch keine Bewertungen
- Presented By: Anlet Jasmine T.M: Protein-Energy MalnutritionDokument24 SeitenPresented By: Anlet Jasmine T.M: Protein-Energy MalnutritionanletNoch keine Bewertungen
- MalnutritionDokument19 SeitenMalnutritionshavonprince97Noch keine Bewertungen
- Handout 1 Intro 2018Dokument57 SeitenHandout 1 Intro 2018Cezhille BattadNoch keine Bewertungen
- Severe Acute MalnutritionDokument42 SeitenSevere Acute MalnutritionEph RemNoch keine Bewertungen
- PEM EPIDEMIOLOGY Classification Prevention and National Health Program India 2020.Dokument78 SeitenPEM EPIDEMIOLOGY Classification Prevention and National Health Program India 2020.psm dataNoch keine Bewertungen
- Protien Energy Malnutrition Nov2008Dokument44 SeitenProtien Energy Malnutrition Nov2008Ivana YolandaNoch keine Bewertungen
- Protein-Calories, Malnutrition & Nutritional DeficienciesDokument15 SeitenProtein-Calories, Malnutrition & Nutritional DeficienciesChino Paolo SamsonNoch keine Bewertungen
- Marasmus - Case ReportDokument13 SeitenMarasmus - Case ReportApriany Cordias Arlita SilalahiNoch keine Bewertungen
- Protein Energy MalnutritionDokument38 SeitenProtein Energy Malnutritionjeshema100% (2)
- Community Nutrition: Prepared By:Mrs Bemina J A Assistant Professor ESIC College of Nursing KalaburagiDokument52 SeitenCommunity Nutrition: Prepared By:Mrs Bemina J A Assistant Professor ESIC College of Nursing Kalaburagibemina ja100% (1)
- Beatrice TukeiDokument9 SeitenBeatrice Tukeisolomonkibet254Noch keine Bewertungen
- Protein-Calories, Malnutrition & Nutritional DeficienciesDokument14 SeitenProtein-Calories, Malnutrition & Nutritional DeficienciesChino Paolo SamsonNoch keine Bewertungen
- Subjects Notes BSC Nursing Part - I (According Inc Syallbus) Subject Nutrition Unit - I Introduction NutritionDokument26 SeitenSubjects Notes BSC Nursing Part - I (According Inc Syallbus) Subject Nutrition Unit - I Introduction NutritionHemant SharmaNoch keine Bewertungen
- MarasmusDokument9 SeitenMarasmusRojanisa Baculi RomathoNoch keine Bewertungen
- Nutritionalproblems Affectingolderadults: Neva L. CroganDokument13 SeitenNutritionalproblems Affectingolderadults: Neva L. CroganALBERTO LUIS LIZCANO GONZALEZ ESTUDIANTENoch keine Bewertungen
- MalnutritionDokument27 SeitenMalnutritionRIYA MARIYATNoch keine Bewertungen
- School of Nursing Science and Research (Sharda University) : Assignment ON Nutritional Problems in CommunityDokument15 SeitenSchool of Nursing Science and Research (Sharda University) : Assignment ON Nutritional Problems in CommunitySamjhana Neupane100% (2)
- Nutritional DiseasesDokument30 SeitenNutritional DiseasesSwara SawantNoch keine Bewertungen
- 3-Malnutrition in Children 2022Dokument27 Seiten3-Malnutrition in Children 2022Emma GumaNoch keine Bewertungen
- Balanced Diet - PPT NewDokument45 SeitenBalanced Diet - PPT NewpixiemedicNoch keine Bewertungen
- Nutrition Through The Lifespan and Diet and Disease BackupDokument67 SeitenNutrition Through The Lifespan and Diet and Disease BackupJessica SnowNoch keine Bewertungen
- Public Health NutritionDokument58 SeitenPublic Health NutritionJaime TaylorNoch keine Bewertungen
- Introduction To Nutrition Contents - Group1Dokument6 SeitenIntroduction To Nutrition Contents - Group1Thea GeronimoNoch keine Bewertungen
- Protein Energy MalnutritionDokument44 SeitenProtein Energy Malnutritionokwadha simionNoch keine Bewertungen
- Pediatrics: Nutritional DisordersDokument4 SeitenPediatrics: Nutritional Disordersapi-3829364Noch keine Bewertungen
- MalnutritionDokument71 SeitenMalnutritionnasibdin100% (2)
- Nutritional Assessment and Malnutrition Under 5 and AboveDokument33 SeitenNutritional Assessment and Malnutrition Under 5 and AboveRamesh kumarNoch keine Bewertungen
- MalnutritionDokument5 SeitenMalnutritionmanishkrvatsNoch keine Bewertungen
- MalnutrionDokument44 SeitenMalnutrionnajeebNoch keine Bewertungen
- Protein Energy Malnutrition: Abdelaziz ElaminDokument49 SeitenProtein Energy Malnutrition: Abdelaziz ElamindocnandiNoch keine Bewertungen
- Nelson's Hour - 58-60Dokument51 SeitenNelson's Hour - 58-60Josselle Sempio CalientaNoch keine Bewertungen
- Nutrition LectureDokument30 SeitenNutrition LectureJovelle Sto.domingoNoch keine Bewertungen
- Nutritional Deficiency Disorder/ (PEM)Dokument37 SeitenNutritional Deficiency Disorder/ (PEM)ShrutiNoch keine Bewertungen
- Malnutrition in The PhilippinesDokument43 SeitenMalnutrition in The PhilippinesOlive Factoriza100% (1)
- 5:2 Diet Cookbook: 5:2 Diet Recipes For Burn Fat Fast, Remove Cellulite, Boost Metabolism & Enjoy Your LifeVon Everand5:2 Diet Cookbook: 5:2 Diet Recipes For Burn Fat Fast, Remove Cellulite, Boost Metabolism & Enjoy Your LifeNoch keine Bewertungen
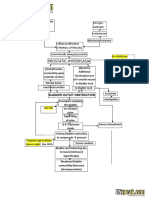
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDokument2 SeitenBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNoch keine Bewertungen
- Borderline CEA (Not Necessary in Pathophysio. Just Present The Table in Sabiston For Discussion)Dokument3 SeitenBorderline CEA (Not Necessary in Pathophysio. Just Present The Table in Sabiston For Discussion)gailNoch keine Bewertungen
- CPG On Chronic CoughDokument93 SeitenCPG On Chronic Coughgail100% (2)
- Right-Sided Colonic Diverticulitis: Clinical Features, Sonographic Appearances, and ManagementDokument7 SeitenRight-Sided Colonic Diverticulitis: Clinical Features, Sonographic Appearances, and ManagementgailNoch keine Bewertungen
- Decison Making RCDDokument3 SeitenDecison Making RCDgailNoch keine Bewertungen
- CKDDokument35 SeitenCKDgailNoch keine Bewertungen
- Pain, Constipation or Abdominal Distension Times Less FrequentDokument3 SeitenPain, Constipation or Abdominal Distension Times Less FrequentgailNoch keine Bewertungen
- Pediatric Basic Life SupportDokument3 SeitenPediatric Basic Life SupportgailNoch keine Bewertungen
- Subcut Mycoses 2012Dokument32 SeitenSubcut Mycoses 2012gailNoch keine Bewertungen
- Endemic Myco2012Dokument49 SeitenEndemic Myco2012gailNoch keine Bewertungen
- 3 Immunology1Dokument317 Seiten3 Immunology1gailNoch keine Bewertungen
- Bacteria Table PrintDokument10 SeitenBacteria Table PrintgailNoch keine Bewertungen
- Increased Increased: Haptoglobin Ceruloplasmin Iron Deficiency AnemiaDokument3 SeitenIncreased Increased: Haptoglobin Ceruloplasmin Iron Deficiency AnemiagailNoch keine Bewertungen
- First Aid For Women and Children PRC June 22 2017 3 To 5 PM PRC LobbyDokument27 SeitenFirst Aid For Women and Children PRC June 22 2017 3 To 5 PM PRC LobbygailNoch keine Bewertungen
- Braunwald S Heart Disease A Textbook of Cardiovascular Medicine Comes To The App Store PDFDokument3 SeitenBraunwald S Heart Disease A Textbook of Cardiovascular Medicine Comes To The App Store PDFgailNoch keine Bewertungen
- Trans - Research - Overview of Evidence Based MedicineDokument2 SeitenTrans - Research - Overview of Evidence Based MedicinegailNoch keine Bewertungen
- Nutrients: Personalized Nutrition Approach in Food Allergy: Is It Prime Time Yet?Dokument16 SeitenNutrients: Personalized Nutrition Approach in Food Allergy: Is It Prime Time Yet?Meisya Nur'ainiNoch keine Bewertungen
- Unit 3: Exercise 1: Match The Activities With The Pictures. Use The Words in The BoxDokument14 SeitenUnit 3: Exercise 1: Match The Activities With The Pictures. Use The Words in The BoxĐoàn Văn Tiến100% (1)
- Sports Nutrition NotesDokument4 SeitenSports Nutrition NotesAudrie Allyson GabalesNoch keine Bewertungen
- Chapter 1 6 Larder 1Dokument32 SeitenChapter 1 6 Larder 1Nawed Khan100% (1)
- The Purchase of Organic Fish in Bangladesh Safeguarding Against COVID-19Dokument30 SeitenThe Purchase of Organic Fish in Bangladesh Safeguarding Against COVID-19Nurul AnisaNoch keine Bewertungen
- Ways of Managing Deficiency DiseasesDokument4 SeitenWays of Managing Deficiency DiseasesMolan JenaNoch keine Bewertungen
- Section 1: About The CategoryDokument29 SeitenSection 1: About The CategoryFilza MaryamNoch keine Bewertungen
- VET & AH EXTENSION UNIT 1 NotesDokument22 SeitenVET & AH EXTENSION UNIT 1 NotesAbhijith S. PNoch keine Bewertungen
- HACCP Basic CourseDokument28 SeitenHACCP Basic CourseHACCPEuropa100% (7)
- Baking Value ChainDokument21 SeitenBaking Value Chainayesha bibiNoch keine Bewertungen
- Hye Doun JanFebMarch 09Dokument12 SeitenHye Doun JanFebMarch 09anrcinfoNoch keine Bewertungen
- What Can You Eat On A Low-Carb Diet? Low-Carb Diets Limit The Number of Carbohydrates ADokument5 SeitenWhat Can You Eat On A Low-Carb Diet? Low-Carb Diets Limit The Number of Carbohydrates ASreeraj RajanNoch keine Bewertungen
- Minimal Processing Technologies in Food IndustryDokument5 SeitenMinimal Processing Technologies in Food IndustryGuadalupe Somera CisnerosNoch keine Bewertungen
- Diet Modified in CompositionDokument34 SeitenDiet Modified in Compositionprecyusman50% (2)
- Cancer Adime NoteDokument4 SeitenCancer Adime Noteapi-299079787Noch keine Bewertungen
- 9-20 Anni FaridahDokument12 Seiten9-20 Anni FaridahJared Delos ReyesNoch keine Bewertungen
- Ayurvedic and Naturopathic Way of Life by Manthena Sathyanarayana RajuDokument7 SeitenAyurvedic and Naturopathic Way of Life by Manthena Sathyanarayana RajuvishnuprakashNoch keine Bewertungen
- Rejuvenation Without Medicines - (Authored by Acharya Shriram Sharma)Dokument47 SeitenRejuvenation Without Medicines - (Authored by Acharya Shriram Sharma)Guiding Thoughts- Books by Pandit Shriram Sharma Acharya100% (3)
- For Better Health: 23 ReasonsDokument2 SeitenFor Better Health: 23 ReasonsNoel TorresNoch keine Bewertungen
- Rice Value Chain Study VietnamDokument367 SeitenRice Value Chain Study VietnamHa NguyenNoch keine Bewertungen
- Which of The Following Statements Best Summarizes The Main Idea of The Passage?Dokument2 SeitenWhich of The Following Statements Best Summarizes The Main Idea of The Passage?Autonomo UsNoch keine Bewertungen
- Satvikk Gifts Catalog 2013 TrentDokument67 SeitenSatvikk Gifts Catalog 2013 TrentiamakingNoch keine Bewertungen
- Neslte Project of HRMDokument21 SeitenNeslte Project of HRMAftab AlamNoch keine Bewertungen
- If Packaging Design Award 2014Dokument2 SeitenIf Packaging Design Award 2014MarketingTribune redactieNoch keine Bewertungen
- PLANT MILK ReportDokument29 SeitenPLANT MILK ReportIvan GarduñoNoch keine Bewertungen
- McDonalds SWOT AnalysisDokument2 SeitenMcDonalds SWOT AnalysisYahya AhmadNoch keine Bewertungen
- Feasibility Study of Soya ProductDokument18 SeitenFeasibility Study of Soya ProductSorabh Dung0% (1)
- Himal 7 2Dokument89 SeitenHimal 7 2abiskarNoch keine Bewertungen
- AnIntroductionToAlchemicalPhilosophy PDFDokument36 SeitenAnIntroductionToAlchemicalPhilosophy PDFdanieladaniela169Noch keine Bewertungen
- Grade 7-12Dokument84 SeitenGrade 7-12Cab VicNoch keine Bewertungen