Das könnte Ihnen auch gefallen
- Fungal Infection - 1Dokument87 SeitenFungal Infection - 1ParamitaNoch keine Bewertungen
- Subcutaneous 06122022Dokument61 SeitenSubcutaneous 06122022Stephano LabiaNoch keine Bewertungen
- Subcutaneous MycosesDokument34 SeitenSubcutaneous MycosesNUBWA MEDUGUNoch keine Bewertungen
- Medical MycologyDokument84 SeitenMedical MycologytenawNoch keine Bewertungen
- GEJALA KLINIK MIKOSIS DAN PENEGAKAN DIAGNOSA LABORATORIUMDokument36 SeitenGEJALA KLINIK MIKOSIS DAN PENEGAKAN DIAGNOSA LABORATORIUMH PNoch keine Bewertungen
- Subcutaneous Mycosis 06-07Dokument16 SeitenSubcutaneous Mycosis 06-07api-3699361100% (1)
- Subcutaneous MycosesDokument14 SeitenSubcutaneous MycosesanonacadsNoch keine Bewertungen
- Subcutaneous MycosesDokument22 SeitenSubcutaneous MycosesIan MosesNoch keine Bewertungen
- Mycology Part 2Dokument215 SeitenMycology Part 2Patricia Jean RodriguezNoch keine Bewertungen
- Week 5. Superficial, Systemic, & Opportunistic MycosesDokument73 SeitenWeek 5. Superficial, Systemic, & Opportunistic MycosesAsdfghjklNoch keine Bewertungen
- Introduction To MycologyDokument46 SeitenIntroduction To MycologyAastha SinhaNoch keine Bewertungen
- Superficial and Cutaneous MycosesDokument34 SeitenSuperficial and Cutaneous MycosesPrincewill Seiyefa100% (1)
- Superficial and Cutaneous Mycoses Diagnosis and TreatmentDokument36 SeitenSuperficial and Cutaneous Mycoses Diagnosis and TreatmentMich BagamanoNoch keine Bewertungen
- Three Types of Fungal Infection (Mycoses)Dokument16 SeitenThree Types of Fungal Infection (Mycoses)Adeleye SamuelNoch keine Bewertungen
- IKD2-K11 - Mikosis Superfisialis, Mikosis Sistemik Dan Mikosis OportunistikDokument64 SeitenIKD2-K11 - Mikosis Superfisialis, Mikosis Sistemik Dan Mikosis OportunistikHalseyNoch keine Bewertungen
- Medically Important FungiDokument57 SeitenMedically Important FungitheprintconerNoch keine Bewertungen
- MycologyDokument68 SeitenMycologyANCHELANoch keine Bewertungen
- Chapter22 LectureDokument45 SeitenChapter22 Lecturecee_prasetyo100% (1)
- Cutaneous and Subcataneous MycosesmDokument15 SeitenCutaneous and Subcataneous MycosesmMaxamed Faarax XaashiNoch keine Bewertungen
- The Fungi of Medical ImportanceDokument44 SeitenThe Fungi of Medical ImportanceBig BrosNoch keine Bewertungen
- Dr.V.Gopalakrishnan's Guide to Medical MycologyDokument41 SeitenDr.V.Gopalakrishnan's Guide to Medical MycologydiniNoch keine Bewertungen
- Opportunistic Mycoses 06-07Dokument35 SeitenOpportunistic Mycoses 06-07api-3699361Noch keine Bewertungen
- 03 Cutaneous MycosesDokument30 Seiten03 Cutaneous MycosesFelix AyornuNoch keine Bewertungen
- Jamur-Jamur Penyebab: Mikosis Superfisial Dermatofitosis Mikosis SubkutanDokument104 SeitenJamur-Jamur Penyebab: Mikosis Superfisial Dermatofitosis Mikosis SubkutanJimmy Fran IINoch keine Bewertungen
- MIKOLOGI Fungal InfectionDokument31 SeitenMIKOLOGI Fungal InfectionAkbar Ahya PutraNoch keine Bewertungen
- Bacterial InfectionDokument122 SeitenBacterial InfectionElga MuralidharanNoch keine Bewertungen
- Cutaneous TuberculosisDokument78 SeitenCutaneous TuberculosisDr Daulat Ram DhakedNoch keine Bewertungen
- Jamur Pada Traktus Respiratorius Asaad Aaa 06 012Dokument58 SeitenJamur Pada Traktus Respiratorius Asaad Aaa 06 012Muhammad Satir SayatiNoch keine Bewertungen
- Subcutaneous MycosesDokument23 SeitenSubcutaneous Mycosessarguss14100% (1)
- Fungal ClassificationDokument109 SeitenFungal ClassificationMirza Shaharyar BaigNoch keine Bewertungen
- Subcutaneous Mycosis: DR Sulaiman ContehDokument17 SeitenSubcutaneous Mycosis: DR Sulaiman ContehAbubakar JallohNoch keine Bewertungen
- Fungal Infections-SubcutaneousDokument24 SeitenFungal Infections-SubcutaneousKato CalebNoch keine Bewertungen
- Foundations in Microbiology: TalaroDokument45 SeitenFoundations in Microbiology: Talaromertx013Noch keine Bewertungen
- Granulo 3Dokument94 SeitenGranulo 3Sathvika BNoch keine Bewertungen
- Sk. Mizanur RahmanDokument24 SeitenSk. Mizanur Rahmanrevathidadam55555Noch keine Bewertungen
- Fungal Infections of the Skin, Hair and NailsDokument120 SeitenFungal Infections of the Skin, Hair and NailsmissirenaNoch keine Bewertungen
- Skin and Soft Tissue Infectons 1Dokument51 SeitenSkin and Soft Tissue Infectons 1AISHWARYA T DNoch keine Bewertungen
- Medically Important Fungal Pathogens (Candida, Aspergillus, CryptococcusDokument17 SeitenMedically Important Fungal Pathogens (Candida, Aspergillus, CryptococcusmeredithNoch keine Bewertungen
- Medical Mycology: DR C. O. Morton Prof. T. R. Rogers Dept of Clinical MicrobiologyDokument40 SeitenMedical Mycology: DR C. O. Morton Prof. T. R. Rogers Dept of Clinical MicrobiologyKhusnul AssidikNoch keine Bewertungen
- Fungal Organisms of Medical Importance: FungiDokument12 SeitenFungal Organisms of Medical Importance: Fungioddone_outNoch keine Bewertungen
- Dimorphic Systemic MycosesDokument65 SeitenDimorphic Systemic Mycoseskedar karkiNoch keine Bewertungen
- BED28 FungiDokument24 SeitenBED28 Fungifira yusufNoch keine Bewertungen
- DIAGNOSTIC MYCOLOGY: SPECIMEN COLLECTION AND IDENTIFICATIONDokument154 SeitenDIAGNOSTIC MYCOLOGY: SPECIMEN COLLECTION AND IDENTIFICATIONJade MonrealNoch keine Bewertungen
- Wound Infection Types, Causes and Fungal DiseasesDokument13 SeitenWound Infection Types, Causes and Fungal DiseasesHabibNoch keine Bewertungen
- Fungal Infection PathologyDokument47 SeitenFungal Infection PathologyJapheth Ouma JumaNoch keine Bewertungen
- Chromo Blas To MycosisDokument51 SeitenChromo Blas To Mycosiskhawar93Noch keine Bewertungen
- Fungal Skin Infections GuideDokument88 SeitenFungal Skin Infections GuideJuan Ortega PutraNoch keine Bewertungen
- Microbial Diseases of The Skin and WoundsDokument34 SeitenMicrobial Diseases of The Skin and WoundsDagnachew kasayeNoch keine Bewertungen
- RED EYE WITH DECREASED VISION FixedDokument70 SeitenRED EYE WITH DECREASED VISION FixedChandraNoch keine Bewertungen
- Cutaneous InfectionsDokument148 SeitenCutaneous InfectionsPratzNoch keine Bewertungen
- Vesicobullous DiseaseDokument40 SeitenVesicobullous Disease65gken100% (1)
- Blood and Tissue ParasitesDokument62 SeitenBlood and Tissue Parasitesapi-3856362Noch keine Bewertungen
- PG - Mycology and Prions. 2020Dokument141 SeitenPG - Mycology and Prions. 2020Omeerul RafieNoch keine Bewertungen
- MycosesDokument28 SeitenMycosesAiman TymerNoch keine Bewertungen
- Mycoses 2022Dokument185 SeitenMycoses 2022esaumulimaNoch keine Bewertungen
- Systemic MycosisDokument62 SeitenSystemic Mycosisrichytum20Noch keine Bewertungen
- In The Name of ALLAH, The Beneficent The MercifulDokument51 SeitenIn The Name of ALLAH, The Beneficent The Mercifulkhawar93Noch keine Bewertungen
- Subcutaneous Mycoses: Presenter: DR Pranay Reddy Moderator: DR Tonita MNDokument81 SeitenSubcutaneous Mycoses: Presenter: DR Pranay Reddy Moderator: DR Tonita MNSandipNoch keine Bewertungen
- Actinomyces & Nocardia 06-07-MedDokument11 SeitenActinomyces & Nocardia 06-07-Medapi-3699361Noch keine Bewertungen
- CPG On Chronic CoughDokument93 SeitenCPG On Chronic Coughgail100% (2)
- WHO Grow Chart TB+U Girl 5-19Dokument1 SeiteWHO Grow Chart TB+U Girl 5-19Kartika AnggakusumaNoch keine Bewertungen
- Z Score BMI 5-19yearsold GirlDokument1 SeiteZ Score BMI 5-19yearsold GirlVienny Widhyanti RosaryaNoch keine Bewertungen
- AP Risk For PerforationDokument7 SeitenAP Risk For PerforationgailNoch keine Bewertungen
- Right-Sided Colonic Diverticulitis: Clinical Features, Sonographic Appearances, and ManagementDokument7 SeitenRight-Sided Colonic Diverticulitis: Clinical Features, Sonographic Appearances, and ManagementgailNoch keine Bewertungen
- Kidney QuizDokument3 SeitenKidney QuizBindashboy0100% (1)
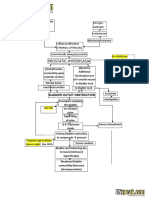
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDokument2 SeitenBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNoch keine Bewertungen
- Cystic Diseases of The KidneyDokument4 SeitenCystic Diseases of The KidneyanxinailofarNoch keine Bewertungen
- 33 Polycystic Kidney DiseaseDokument2 Seiten33 Polycystic Kidney Diseasemurali_bharadwaz100% (1)
- Nursing Care Plan - Pneumothorax PDFDokument2 SeitenNursing Care Plan - Pneumothorax PDFJanine Joy Orpilla76% (25)
- Borderline CEA (Not Necessary in Pathophysio. Just Present The Table in Sabiston For Discussion)Dokument3 SeitenBorderline CEA (Not Necessary in Pathophysio. Just Present The Table in Sabiston For Discussion)gailNoch keine Bewertungen
- Olonic Iverticulitis in The LderlyDokument7 SeitenOlonic Iverticulitis in The LderlygailNoch keine Bewertungen
- Body Defenses & Immunity: But If Skin Is Moist, Not Cleaned Frequently EnoughDokument10 SeitenBody Defenses & Immunity: But If Skin Is Moist, Not Cleaned Frequently EnoughSherwann Vergara Delos ReyesNoch keine Bewertungen
- AP Vs DCDokument11 SeitenAP Vs DCgailNoch keine Bewertungen
- GIT BleedingDokument7 SeitenGIT BleedinggailNoch keine Bewertungen
- Decison Making RCDDokument3 SeitenDecison Making RCDgailNoch keine Bewertungen
- Pain, Constipation or Abdominal Distension Times Less FrequentDokument3 SeitenPain, Constipation or Abdominal Distension Times Less FrequentgailNoch keine Bewertungen
- Pediatric Basic Life Support TechniquesDokument3 SeitenPediatric Basic Life Support TechniquesgailNoch keine Bewertungen
- Endemic Mycoses: Four Primary Fungal InfectionsDokument49 SeitenEndemic Mycoses: Four Primary Fungal InfectionsgailNoch keine Bewertungen
- Immunology Study: Host Reactions to Foreign SubstancesDokument317 SeitenImmunology Study: Host Reactions to Foreign SubstancesgailNoch keine Bewertungen
- Concise overview of chronic kidney disease (CKDDokument35 SeitenConcise overview of chronic kidney disease (CKDgailNoch keine Bewertungen
- Bacteria Table PrintDokument10 SeitenBacteria Table PrintgailNoch keine Bewertungen
- Nutritiona L Disorders: Paulette Benjamin-Chin MD Diplomate, Philippine Pediatric SocietyDokument102 SeitenNutritiona L Disorders: Paulette Benjamin-Chin MD Diplomate, Philippine Pediatric SocietygailNoch keine Bewertungen
- Haptoglobin Ceruloplasmin A2-macroglobin Transferrin biomarkersDokument3 SeitenHaptoglobin Ceruloplasmin A2-macroglobin Transferrin biomarkersgailNoch keine Bewertungen
- First Aid For Injuries, Bleeding and Wounds PCFM 1 Janaury 15 2018Dokument55 SeitenFirst Aid For Injuries, Bleeding and Wounds PCFM 1 Janaury 15 2018gailNoch keine Bewertungen
- PCFM 2 Water Pollution Lecture With DENR Combine 2018 PDFDokument95 SeitenPCFM 2 Water Pollution Lecture With DENR Combine 2018 PDFgailNoch keine Bewertungen
- First Aid For Women and Children PRC June 22 2017 3 To 5 PM PRC LobbyDokument27 SeitenFirst Aid For Women and Children PRC June 22 2017 3 To 5 PM PRC LobbygailNoch keine Bewertungen
- Short-Term Clinical Outcomes and Safety Associated With Percutaneous Radiofrequency Treatment For Excessive SweatingDokument10 SeitenShort-Term Clinical Outcomes and Safety Associated With Percutaneous Radiofrequency Treatment For Excessive SweatingsadraNoch keine Bewertungen
- Meniscus Disorders, Knee: The Medical Disability Advisor: Workplace Guidelines For Disability DurationDokument5 SeitenMeniscus Disorders, Knee: The Medical Disability Advisor: Workplace Guidelines For Disability DurationStephen Nathaniel100% (1)
- Medicina Paliativa Walsh - Comprimido PDFDokument1.507 SeitenMedicina Paliativa Walsh - Comprimido PDFMaría Isabel GarcíaNoch keine Bewertungen
- CH13 Ninenth Standard NCERT BOOKDokument26 SeitenCH13 Ninenth Standard NCERT BOOKPrash ShanthNoch keine Bewertungen
- Format OpnameDokument21 SeitenFormat OpnamerestutiyanaNoch keine Bewertungen
- Final Thesis Abdi Majid Mohamed HassanDokument26 SeitenFinal Thesis Abdi Majid Mohamed HassanAbdi Majid Mohamed Hassan100% (1)
- List of Reference BooksDokument2 SeitenList of Reference BooksShagorShagorNoch keine Bewertungen
- NHS LA - Duty of Candour 2014 - SlidesDokument10 SeitenNHS LA - Duty of Candour 2014 - SlidesAgnieszka WaligóraNoch keine Bewertungen
- Drug Name Mechanism of Action Indication Contraindication Side Effects Nursing Responsibility Generic NameDokument4 SeitenDrug Name Mechanism of Action Indication Contraindication Side Effects Nursing Responsibility Generic NameDan HizonNoch keine Bewertungen
- Top 100 Study Items For The Otolaryngology (ENT) Board ExaminationDokument8 SeitenTop 100 Study Items For The Otolaryngology (ENT) Board ExaminationsduxNoch keine Bewertungen
- Cytokine StormDokument1 SeiteCytokine StormLNoch keine Bewertungen
- Region Name of LaboratoryDokument7 SeitenRegion Name of LaboratorySabling DritzcNoch keine Bewertungen
- Alcoholic Gastritis Case PresentationDokument18 SeitenAlcoholic Gastritis Case Presentationstancy thomas100% (1)
- Clean Room SpecificationsDokument2 SeitenClean Room SpecificationsAli KureishiNoch keine Bewertungen
- Autism Spectrum DisorderDokument14 SeitenAutism Spectrum DisorderAngie McaNoch keine Bewertungen
- Concussions PowerpointDokument15 SeitenConcussions Powerpointapi-240817936Noch keine Bewertungen
- Timing of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyDokument3 SeitenTiming of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyJuan J. Acosta VelásquezNoch keine Bewertungen
- Cambridge OET AnswersDokument11 SeitenCambridge OET AnswersNimraj Patel100% (3)
- Theme 1 - Historic Transitions and Emergence of Epidemic Infections-EnDokument3 SeitenTheme 1 - Historic Transitions and Emergence of Epidemic Infections-EnRichard PriorNoch keine Bewertungen
- POC CHWO HW Solutions PDFDokument5 SeitenPOC CHWO HW Solutions PDFakashkr619Noch keine Bewertungen
- Pictotrans: Pathology of The Breast Quiz From Dra. Edna May Lasap-GoDokument32 SeitenPictotrans: Pathology of The Breast Quiz From Dra. Edna May Lasap-Go2012Noch keine Bewertungen
- Clinical Aspect of Exercise PhysiologyDokument34 SeitenClinical Aspect of Exercise PhysiologyAnn LoricaNoch keine Bewertungen
- Ryan Tarr RN ResumeDokument1 SeiteRyan Tarr RN Resumeapi-456377205Noch keine Bewertungen
- Bag-Mask Ventillation PDFDokument6 SeitenBag-Mask Ventillation PDFHaris PapadopoulosNoch keine Bewertungen
- 01 A History of The Pharmaceutical IndustryDokument8 Seiten01 A History of The Pharmaceutical IndustryHayat NaqviNoch keine Bewertungen
- Understanding Anemia: Causes, Symptoms, Diagnosis and TreatmentDokument27 SeitenUnderstanding Anemia: Causes, Symptoms, Diagnosis and Treatment1108010091Noch keine Bewertungen
- HaemoparasitesDokument82 SeitenHaemoparasitesAshok WiselinNoch keine Bewertungen
- Katzung - Basic and Clinical Pharmacology 12th Edition (2012) PDFDokument8 SeitenKatzung - Basic and Clinical Pharmacology 12th Edition (2012) PDFAl Aleem0% (2)
- Collection of Clean Catch Urine SpecimenDokument21 SeitenCollection of Clean Catch Urine Specimendeonrey1989100% (1)
- Mount Sinai Expert Guides Critical Care - (Part 3 Pulmonary Critical Care)Dokument13 SeitenMount Sinai Expert Guides Critical Care - (Part 3 Pulmonary Critical Care)ShawnNoch keine Bewertungen