Das könnte Ihnen auch gefallen
- MEDICAL STUDENTS and DOCTORS WORLD Nursing Mnemonics Best Collection For StudentsDokument11 SeitenMEDICAL STUDENTS and DOCTORS WORLD Nursing Mnemonics Best Collection For Studentsgovind_soni_15Noch keine Bewertungen
- Prevention & Identification: Skin CancerDokument25 SeitenPrevention & Identification: Skin Cancermkman100% (1)
- Penile Squamous Cell CarcinomaDokument64 SeitenPenile Squamous Cell CarcinomaTres De GuzmanNoch keine Bewertungen
- The AbdomenDokument3 SeitenThe AbdomenotaNoch keine Bewertungen
- Squamous Cell CarcinomaDokument29 SeitenSquamous Cell CarcinomaAswad AffandiNoch keine Bewertungen
- Degenerative Disease The Biology of Skin CancerDokument40 SeitenDegenerative Disease The Biology of Skin CancerRini Agustin IdrisNoch keine Bewertungen
- 6 Endometrial Polyp - Libre PathologyDokument4 Seiten6 Endometrial Polyp - Libre PathologyfadoNoch keine Bewertungen
- Patho5-10 - Male Genitalia (Dr. Villamayor)Dokument8 SeitenPatho5-10 - Male Genitalia (Dr. Villamayor)Miguel Cuevas DolotNoch keine Bewertungen
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDokument27 SeitenCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3Noch keine Bewertungen
- Squamous Cell Skin CancerDokument2 SeitenSquamous Cell Skin CancerToni Mas IrwandaNoch keine Bewertungen
- Function of Git System:: Pepsinogen, Increases Gastric Blood Flow, Stimulates Gastric Smooth Muscle ContractionDokument9 SeitenFunction of Git System:: Pepsinogen, Increases Gastric Blood Flow, Stimulates Gastric Smooth Muscle ContractionRovefrances ErpeluaNoch keine Bewertungen
- Grading and Staging of TumorsDokument11 SeitenGrading and Staging of TumorsJahanzaib Bashir100% (1)
- AntiCancer DrugsDokument21 SeitenAntiCancer Drugssk100% (1)
- Megaloblastic Anemias: Dept of Medicine AcmsDokument71 SeitenMegaloblastic Anemias: Dept of Medicine Acmskunal ghosh100% (1)
- Iron Metabolism: DR Mukhtiar BaigDokument58 SeitenIron Metabolism: DR Mukhtiar BaigdrmukhtiarbaigNoch keine Bewertungen
- Reported By: Porlas, Mary Josephine N. BN41Dokument15 SeitenReported By: Porlas, Mary Josephine N. BN41matrixtrinity100% (1)
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Dokument41 SeitenGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNoch keine Bewertungen
- Mrs - Lakshmi Aged 54 Years Who Is A Flower Seller Residing atDokument5 SeitenMrs - Lakshmi Aged 54 Years Who Is A Flower Seller Residing atHariNoch keine Bewertungen
- Acute PancreatitisDokument46 SeitenAcute PancreatitisLew NianNoch keine Bewertungen
- Cardio NotesDokument2 SeitenCardio NotesMagdaraog Gabrielle A.Noch keine Bewertungen
- Acute Tubular NecrosisDokument60 SeitenAcute Tubular NecrosisYedesney C. LinaresNoch keine Bewertungen
- A&P - 2. Functional Anatomy of The Urinary System (9p)Dokument9 SeitenA&P - 2. Functional Anatomy of The Urinary System (9p)Kris GulleyNoch keine Bewertungen
- Renal PathologyDokument49 SeitenRenal PathologyQusaiBadrNoch keine Bewertungen
- Gastrointestinal and Endocrine Disorder HandoutsDokument120 SeitenGastrointestinal and Endocrine Disorder HandoutsJan Michael R. RemoladoNoch keine Bewertungen
- Medical Pathology Ii. Pathology of Urinary System Lectuer NotesDokument26 SeitenMedical Pathology Ii. Pathology of Urinary System Lectuer Noteseric epahNoch keine Bewertungen
- Dermatology Primer: Selected Skin Diseases and TreatmentDokument87 SeitenDermatology Primer: Selected Skin Diseases and TreatmentArfyanda Aan100% (1)
- Dr. ChintanDokument60 SeitenDr. ChintanWaqar AhmedNoch keine Bewertungen
- Presented By: DR Sharmila G SDokument76 SeitenPresented By: DR Sharmila G SSharmila Shivakumar G SNoch keine Bewertungen
- Structural Biology of HIVDokument31 SeitenStructural Biology of HIVLaura TapiaNoch keine Bewertungen
- ANA213 - Urinary System - AY2020-2021 PDFDokument42 SeitenANA213 - Urinary System - AY2020-2021 PDFSairelle Sordilla ObangNoch keine Bewertungen
- Nervous System NotesDokument13 SeitenNervous System Noteschryan1989100% (1)
- Diagn Approach of Abdominal PainDokument53 SeitenDiagn Approach of Abdominal PainNuriNoch keine Bewertungen
- Lecture 1 - Introduction To HematologyDokument30 SeitenLecture 1 - Introduction To Hematologyimam100% (1)
- Hepatobiliary DiseaseDokument60 SeitenHepatobiliary DiseaseFirdaus AslamNoch keine Bewertungen
- A&P 302 GI:Digestive System Lecture NotesDokument51 SeitenA&P 302 GI:Digestive System Lecture NotesBethanyNoch keine Bewertungen
- Cerebral Blood FlowDokument39 SeitenCerebral Blood FlowRajat ThakurNoch keine Bewertungen
- Skin Cancer SurgeryDokument2 SeitenSkin Cancer SurgeryContinuum Hospitals of New York100% (1)
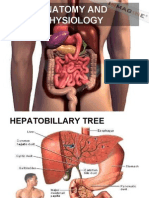
- Anatomy and PhysiologyDokument24 SeitenAnatomy and PhysiologyGillarhymesNoch keine Bewertungen
- Anat 6.3 GSA Appendix - EsguerraDokument4 SeitenAnat 6.3 GSA Appendix - Esguerralovelots1234Noch keine Bewertungen
- Embryo NotesDokument52 SeitenEmbryo NotesSharona Avgush100% (1)
- 17 - Gallbladder StonesDokument71 Seiten17 - Gallbladder StonesRashed Shatnawi100% (1)
- General Pathology 4.03 Endocrine System Super SummaryDokument15 SeitenGeneral Pathology 4.03 Endocrine System Super SummaryJade MonrealNoch keine Bewertungen
- Anatomy and Physiology - Kidney - ForDokument3 SeitenAnatomy and Physiology - Kidney - ForKristelle ModalesNoch keine Bewertungen
- Anatomy of The Liver and Biliary SystemDokument11 SeitenAnatomy of The Liver and Biliary Systemapi-372329083% (6)
- Histology of Lower GITDokument27 SeitenHistology of Lower GITArwa100% (2)
- Skin CancerDokument37 SeitenSkin CancerSangita Sonwane100% (1)
- 12 - Hemostasis 1Dokument21 Seiten12 - Hemostasis 1جووري جووري100% (1)
- Obstructive Jaundice: DR Nanteza SumayiyaDokument26 SeitenObstructive Jaundice: DR Nanteza SumayiyaNinaNoch keine Bewertungen
- Hematology Pathology - 002) CBC - Approach To Polycythemia (Notes)Dokument4 SeitenHematology Pathology - 002) CBC - Approach To Polycythemia (Notes)Aro DanaNoch keine Bewertungen
- History Taking: Item DescriptionDokument22 SeitenHistory Taking: Item DescriptionBikash Sah100% (1)
- Physiology of The Gastrointestinal Tract (Git)Dokument98 SeitenPhysiology of The Gastrointestinal Tract (Git)jballungayNoch keine Bewertungen
- Coronary Artery DiseaseDokument7 SeitenCoronary Artery Diseasejmar767Noch keine Bewertungen
- β-Lactam Antibiotics: carbapenemsDokument14 Seitenβ-Lactam Antibiotics: carbapenemsim. EliasNoch keine Bewertungen
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDokument5 SeitenPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzNoch keine Bewertungen
- Pathology B - Gastrointestinal Tract (Esguerra, 2015) PDFDokument18 SeitenPathology B - Gastrointestinal Tract (Esguerra, 2015) PDFJem QuintoNoch keine Bewertungen
- Patho. Reviewer On Cellular InjuryDokument21 SeitenPatho. Reviewer On Cellular InjurySeff CausapinNoch keine Bewertungen
- JaundiceDokument53 SeitenJaundiceAbhishiktaAbhiNoch keine Bewertungen
- 3-Major Veins of The BodyDokument26 Seiten3-Major Veins of The BodyTJPlayz100% (1)
- 2 - Kuliah Fisiologi - Balqis, DRDokument118 Seiten2 - Kuliah Fisiologi - Balqis, DRRachmania BudiatiNoch keine Bewertungen
- GitDokument57 SeitenGitbookaccountNoch keine Bewertungen
- HD Management Brochure - Final PDFDokument2 SeitenHD Management Brochure - Final PDFVanzari RBMNoch keine Bewertungen
- API 572 Practise QuestionDokument58 SeitenAPI 572 Practise Questionbelonk_182100% (6)
- Security Officer Part Time in Orange County CA Resume Robert TalleyDokument2 SeitenSecurity Officer Part Time in Orange County CA Resume Robert TalleyRobertTalleyNoch keine Bewertungen
- Abrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition Test BankDokument6 SeitenAbrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition Test BankWilliam Nakken100% (28)
- Disease PreventionDokument14 SeitenDisease PreventionJoan InsonNoch keine Bewertungen
- DENSO Diagnostic TipsDokument1 SeiteDENSO Diagnostic TipsVerona MamaiaNoch keine Bewertungen
- ASTM Standards For WoodDokument7 SeitenASTM Standards For WoodarslanengNoch keine Bewertungen
- TNEB Thermal Power PlantDokument107 SeitenTNEB Thermal Power Plantvicky_hyd_130% (1)
- Amirtha ProjectDokument18 SeitenAmirtha Projectaeriel judson100% (1)
- Genie PDFDokument264 SeitenGenie PDFjohanaNoch keine Bewertungen
- How Condensing Boilers WorkDokument1 SeiteHow Condensing Boilers WorkBrianNoch keine Bewertungen
- Drug StudyDokument4 SeitenDrug Studysnowyfingers100% (1)
- Hygold 5000Bs: Base Oil Marketing SpecificationDokument1 SeiteHygold 5000Bs: Base Oil Marketing Specificationsamsoon80100% (1)
- Indian Income Tax Return Acknowledgement: Do Not Send This Acknowledgement To CPC, BengaluruDokument1 SeiteIndian Income Tax Return Acknowledgement: Do Not Send This Acknowledgement To CPC, BengaluruDrsex DrsexNoch keine Bewertungen
- Clase No. 24 Nouns and Their Modifiers ExercisesDokument2 SeitenClase No. 24 Nouns and Their Modifiers ExercisesenriquefisicoNoch keine Bewertungen
- Bradycardia AlgorithmDokument1 SeiteBradycardia AlgorithmGideon BahuleNoch keine Bewertungen
- Case StudyDokument3 SeitenCase StudyMarlon MagtibayNoch keine Bewertungen
- FACSDokument8 SeitenFACSKarthick ThiyagarajanNoch keine Bewertungen
- Biecco Lawrie Ece Gec Reyrolle Burn Jyoti SwitchgearDokument18 SeitenBiecco Lawrie Ece Gec Reyrolle Burn Jyoti SwitchgearSharafat AliNoch keine Bewertungen
- IJARIE Paper 17936 PDFDokument7 SeitenIJARIE Paper 17936 PDFArbelyn RoblesNoch keine Bewertungen
- Acc030 Financial Statement & Income Statement FormatDokument2 SeitenAcc030 Financial Statement & Income Statement FormatAqilahNoch keine Bewertungen
- The Daily Star On 19.05.2021Dokument12 SeitenThe Daily Star On 19.05.2021nira miraNoch keine Bewertungen
- Fpubh 10 1079779Dokument10 SeitenFpubh 10 1079779Dona WirdaningsiNoch keine Bewertungen
- Major Laishram Jyotin SinghDokument3 SeitenMajor Laishram Jyotin SinghSpongebob SquarepantsNoch keine Bewertungen
- Implementation Plan SLRPDokument6 SeitenImplementation Plan SLRPAngelina SantosNoch keine Bewertungen
- Service Manual SM1-76-38.0: Collector Ring, ReconditionDokument4 SeitenService Manual SM1-76-38.0: Collector Ring, ReconditionJorge YuniorNoch keine Bewertungen
- KorfundDokument68 SeitenKorfundnhy.mail2709100% (1)
- Saving AccountDokument9 SeitenSaving AccountpalkhinNoch keine Bewertungen
- Kristen Swanson's Theory of CaringDokument12 SeitenKristen Swanson's Theory of CaringAlexandria David50% (2)
- Cameron Scanner 2000 Hardware User Manual PDFDokument11 SeitenCameron Scanner 2000 Hardware User Manual PDFPes SilvaNoch keine Bewertungen