Das könnte Ihnen auch gefallen
- The Slim Book of Health Pearls: Symptoms Never to IgnoreVon EverandThe Slim Book of Health Pearls: Symptoms Never to IgnoreNoch keine Bewertungen
- History/Physical and Symptoms and Signs of Different Diseases in UrologyDokument26 SeitenHistory/Physical and Symptoms and Signs of Different Diseases in UrologyDr. NasrumminallahNoch keine Bewertungen
- Acute and Chronic Urinary RetentionDokument3 SeitenAcute and Chronic Urinary RetentionParyNoch keine Bewertungen
- UTIs 1Dokument38 SeitenUTIs 1Eduardo Valdez RodríguezNoch keine Bewertungen
- Renal Notes Step 2ckDokument34 SeitenRenal Notes Step 2cksamreen100% (1)
- Types of Incontinence: Pertinent Negatives? Fever Chills Malaise Dysuria Perineal or Rectal PainDokument4 SeitenTypes of Incontinence: Pertinent Negatives? Fever Chills Malaise Dysuria Perineal or Rectal PainDanekka TanNoch keine Bewertungen
- Presentation On Dysuria 1Dokument25 SeitenPresentation On Dysuria 1ankur acharyaNoch keine Bewertungen
- Urinary & Renal Deviations: Edited By: Cynthia Bartlau, MSN, RN, PHNDokument60 SeitenUrinary & Renal Deviations: Edited By: Cynthia Bartlau, MSN, RN, PHNmolyebeedNoch keine Bewertungen
- Key Urological SymptomsDokument25 SeitenKey Urological SymptomsStella Agatha WidjajaNoch keine Bewertungen
- History and Examination of Urologenital SystemDokument29 SeitenHistory and Examination of Urologenital SystemPrincewill SeiyefaNoch keine Bewertungen
- Elderly Urinary Tract Disorders FixDokument36 SeitenElderly Urinary Tract Disorders FixRyan Adi PutraNoch keine Bewertungen
- Nursing Care Plans For UTIDokument2 SeitenNursing Care Plans For UTIHannah Pin67% (3)
- Urinary Tract InfectionsDokument71 SeitenUrinary Tract Infectionsdayibon499Noch keine Bewertungen
- Acute and Chronic PyelonephritisDokument7 SeitenAcute and Chronic PyelonephritisMatthew Ryan100% (1)
- BPH and Urethral StrictureDokument25 SeitenBPH and Urethral Stricturezaminazz100% (1)
- Urinary Tract DisordersDokument54 SeitenUrinary Tract Disorderssharon ocharaNoch keine Bewertungen
- Renal and Urinary DisordersDokument134 SeitenRenal and Urinary Disordersmirmodepon05100% (1)
- Urinary IncontinenceDokument12 SeitenUrinary IncontinenceAmrit Preet KaurNoch keine Bewertungen
- Urology HX and ExamDokument31 SeitenUrology HX and ExamMisbah KaleemNoch keine Bewertungen
- Medical SurgicalDokument30 SeitenMedical SurgicalGulshad AfridiNoch keine Bewertungen
- Benign Prostatic Hypertrophy - ClinicalKeyDokument24 SeitenBenign Prostatic Hypertrophy - ClinicalKeyJhosept Perez AlvaNoch keine Bewertungen
- Urinary Tract Infection (UTI) in Males: Signs and SymptomsDokument33 SeitenUrinary Tract Infection (UTI) in Males: Signs and Symptomssyak turNoch keine Bewertungen
- Urinary Retention 2Dokument3 SeitenUrinary Retention 2Agli AdhityaNoch keine Bewertungen
- What Is Acute PyelonephritisDokument2 SeitenWhat Is Acute PyelonephritisAnnabel Dela CruzNoch keine Bewertungen
- Case Study On Bilateral NephrolithiasisDokument84 SeitenCase Study On Bilateral NephrolithiasisSteph BulanNoch keine Bewertungen
- Genito Urinary SystemDokument10 SeitenGenito Urinary SystemArul ValanNoch keine Bewertungen
- Diseases of Urogenital TractDokument170 SeitenDiseases of Urogenital TractMuhammadNoch keine Bewertungen
- Medical-Surgical Nursing: An Integrated Approach, 2EDokument38 SeitenMedical-Surgical Nursing: An Integrated Approach, 2Eegan_erlinNoch keine Bewertungen
- ####Bahan Kuliah ISK Blok 23 (Nov 2015)Dokument32 Seiten####Bahan Kuliah ISK Blok 23 (Nov 2015)ajengdmrNoch keine Bewertungen
- Renal Disorders 1Dokument73 SeitenRenal Disorders 1Kyla PamaNoch keine Bewertungen
- Disease of Prostate Tutorial-Dec-2014Dokument49 SeitenDisease of Prostate Tutorial-Dec-2014marina_shawkyNoch keine Bewertungen
- Male Reproductive DisordersDokument5 SeitenMale Reproductive DisorderslordwinjohnbernardoNoch keine Bewertungen
- Pelvic Anatomy Slides FINALDokument36 SeitenPelvic Anatomy Slides FINALRajashekharNoch keine Bewertungen
- UtiDokument23 SeitenUtiShamila KaruthuNoch keine Bewertungen
- Benign Prostatic Hyperplasia (BPH) and Bladder Outlet Obstruction (BOO)Dokument73 SeitenBenign Prostatic Hyperplasia (BPH) and Bladder Outlet Obstruction (BOO)Swe Zin NaingNoch keine Bewertungen
- Female Urinary Retention - StatPearls - NCBI BookshelfDokument26 SeitenFemale Urinary Retention - StatPearls - NCBI BookshelfjqgjwgnnwkNoch keine Bewertungen
- Acute Appendicitis: Patan Academy of Health SciencesDokument10 SeitenAcute Appendicitis: Patan Academy of Health Sciencessuman subediNoch keine Bewertungen
- Urinary System DisordersDokument14 SeitenUrinary System DisordersGideon P. CasasNoch keine Bewertungen
- 10urogenital DiseaseDokument24 Seiten10urogenital DiseaseAli SherNoch keine Bewertungen
- Benign Prostatic HyperplasiaDokument19 SeitenBenign Prostatic HyperplasiaEmmanuel MacheleleNoch keine Bewertungen
- History and Physical Exam For The Urologic PatientDokument39 SeitenHistory and Physical Exam For The Urologic PatientNendy OktariNoch keine Bewertungen
- Ou Sumber4Dokument14 SeitenOu Sumber4AnggaNoch keine Bewertungen
- Urologic ExaminationDokument4 SeitenUrologic ExaminationTansanee MalivalayaNoch keine Bewertungen
- Urinary Tract Obstruction: Zheng Xuepei MDDokument66 SeitenUrinary Tract Obstruction: Zheng Xuepei MDapi-19916399Noch keine Bewertungen
- Clinical Examination of Genitourinary SystemDokument43 SeitenClinical Examination of Genitourinary SystemKeamina .aNoch keine Bewertungen
- UrologyDokument35 SeitenUrologymiansk100% (1)
- Wa0038.Dokument5 SeitenWa0038.sham gowliNoch keine Bewertungen
- Infectious and Inflammatory Disorders of The Urinary SystemDokument16 SeitenInfectious and Inflammatory Disorders of The Urinary SystemBibi Renu100% (1)
- Symptoms: For Bladder InfectionsDokument5 SeitenSymptoms: For Bladder InfectionsGene Ryuzaki SeseNoch keine Bewertungen
- Assessment of Renal and Urinary Tract FunctionDokument40 SeitenAssessment of Renal and Urinary Tract FunctionBjorn Francisco100% (1)
- Uti 1Dokument75 SeitenUti 1Muwanga faizoNoch keine Bewertungen
- Acuteurologicalconditions 130121123140 Phpapp01Dokument58 SeitenAcuteurologicalconditions 130121123140 Phpapp01Dr. NasrumminallahNoch keine Bewertungen
- HX Taking Reproductive SystemDokument78 SeitenHX Taking Reproductive SystemMuskaan ZaharaNoch keine Bewertungen
- Clinical Case HomeworkDokument4 SeitenClinical Case HomeworkIris BakerNoch keine Bewertungen
- Urinary IncontinenceDokument17 SeitenUrinary IncontinenceMohamed Na3eemNoch keine Bewertungen
- Chapter 45 Urinary EliminationDokument29 SeitenChapter 45 Urinary EliminationKwenaNoch keine Bewertungen
- Asymptomatic BacteriuriaDokument23 SeitenAsymptomatic BacteriuriaSabita PaudelNoch keine Bewertungen
- Urinary Disorders 2Dokument19 SeitenUrinary Disorders 2ula mdiNoch keine Bewertungen
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesVon EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesBewertung: 5 von 5 Sternen5/5 (2)
- Penile CancerDokument58 SeitenPenile CancerPatrascu CristiNoch keine Bewertungen
- C18 - Edemul Pulmonar AcutDokument25 SeitenC18 - Edemul Pulmonar AcutDascal RalucaNoch keine Bewertungen
- C4-5 - Bolile ValvulareDokument27 SeitenC4-5 - Bolile ValvulareAnda Madalina ZahariaNoch keine Bewertungen
- C15 - PericarditeDokument30 SeitenC15 - PericarditeAnda Madalina ZahariaNoch keine Bewertungen
- Urologyppt 1217856119824899 8Dokument130 SeitenUrologyppt 1217856119824899 8Patrascu CristiNoch keine Bewertungen
- Urinary Tract Anatomy and Relevant PathologyDokument28 SeitenUrinary Tract Anatomy and Relevant PathologyDr. NasrumminallahNoch keine Bewertungen
- Urinary Incontinence: Guidelines OnDokument52 SeitenUrinary Incontinence: Guidelines OnPatrascu CristiNoch keine Bewertungen
- 23 PDFDokument90 Seiten23 PDFPatrascu CristiNoch keine Bewertungen
- Kidney Stones: Kim Applebee Alex KaullenDokument26 SeitenKidney Stones: Kim Applebee Alex KaullenPatrascu CristiNoch keine Bewertungen
- Guidelines On: Paediatric UrologyDokument72 SeitenGuidelines On: Paediatric UrologyPatrascu CristiNoch keine Bewertungen
- Guidelines On: Chronic Pelvic PainDokument90 SeitenGuidelines On: Chronic Pelvic PainPatrascu CristiNoch keine Bewertungen
- EAU Pocket Guidelines 215 Edn.Dokument369 SeitenEAU Pocket Guidelines 215 Edn.Mohammed HusseinNoch keine Bewertungen
- Reference RepositoryDokument1 SeiteReference RepositoryPatrascu CristiNoch keine Bewertungen
- Neurogenic Lower Urinary Tract Dysfunction: Guidelines OnDokument52 SeitenNeurogenic Lower Urinary Tract Dysfunction: Guidelines OnPatrascu CristiNoch keine Bewertungen
- Antibiotic eDokument50 SeitenAntibiotic ePatrascu CristiNoch keine Bewertungen
- Guidelines On: Male InfertilityDokument62 SeitenGuidelines On: Male InfertilityPatrascu CristiNoch keine Bewertungen
- Male Sexual Dysfunction:: Guidelines OnDokument49 SeitenMale Sexual Dysfunction:: Guidelines OnPatrascu CristiNoch keine Bewertungen
- Fish - Fabiano Cystoscopy and UreterosDokument8 SeitenFish - Fabiano Cystoscopy and UreterosPatrascu CristiNoch keine Bewertungen
- Pain Scales and Assessment UnhasDokument93 SeitenPain Scales and Assessment Unhashaphahap0% (1)
- The Fun Way To Learn EnglishDokument7 SeitenThe Fun Way To Learn EnglishPatrascu CristiNoch keine Bewertungen
- Concept PaperDokument1 SeiteConcept PaperKurt NicolasNoch keine Bewertungen
- Indonesia Health SectorDokument84 SeitenIndonesia Health SectorBung RandiNoch keine Bewertungen
- Surgery PyqDokument17 SeitenSurgery PyqPrateek SinghNoch keine Bewertungen
- Artrite REATIVAsexualmente ADQUIRIDADokument10 SeitenArtrite REATIVAsexualmente ADQUIRIDAYgor AlbuquerqueNoch keine Bewertungen
- Summary Chart Us Medical Eligibility Criteria - 508taggedDokument2 SeitenSummary Chart Us Medical Eligibility Criteria - 508taggedsanjeev thadaniNoch keine Bewertungen
- Damage Control Fixation of Displaced Femoral.10Dokument6 SeitenDamage Control Fixation of Displaced Femoral.10Hizkyas KassayeNoch keine Bewertungen
- of PHDDokument129 Seitenof PHDHimanshu GargNoch keine Bewertungen
- Clindamycin - ClinicalKeyDokument78 SeitenClindamycin - ClinicalKeyTRI SETYA NINGSIHNoch keine Bewertungen
- Hiv Informative Genre FinalDokument9 SeitenHiv Informative Genre Finalapi-510346047Noch keine Bewertungen
- What Is LoveDokument23 SeitenWhat Is Loveelisabeth cindyNoch keine Bewertungen
- Writers Cramp - A Major Conundrum: Review Article44Dokument7 SeitenWriters Cramp - A Major Conundrum: Review Article44IJAR JOURNALNoch keine Bewertungen
- Inside StoryDokument3 SeitenInside StoryAutismeyeNoch keine Bewertungen
- Treatment DurationDokument7 SeitenTreatment DurationTRI SETYA NINGSIHNoch keine Bewertungen
- Gambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusDokument6 SeitenGambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusRizka ZahroNoch keine Bewertungen
- Aids HivDokument140 SeitenAids HivKarina Flores RezpkaNoch keine Bewertungen
- Opportunistic Fungal Infection PDFDokument48 SeitenOpportunistic Fungal Infection PDFMalvika BabuNoch keine Bewertungen
- International Health RegulationDokument60 SeitenInternational Health RegulationAnonymous 7ugfwjsHQUNoch keine Bewertungen
- Electron Cryotomography of SARS-CoV-2 VirionsDokument1 SeiteElectron Cryotomography of SARS-CoV-2 VirionsIsmaelMendozaNoch keine Bewertungen
- Pengaruh Senam Kaki Terhadap Kadar Glukosa Darah Dan Nilai ABI Penderita DMDokument6 SeitenPengaruh Senam Kaki Terhadap Kadar Glukosa Darah Dan Nilai ABI Penderita DMSetyardiNoch keine Bewertungen
- Malaria in Pregnancy. NewDokument23 SeitenMalaria in Pregnancy. Newgloriashirima8Noch keine Bewertungen
- Family Laboratory For Medical Analysis: Test & SpecimenDokument1 SeiteFamily Laboratory For Medical Analysis: Test & SpecimenMohamad BadranNoch keine Bewertungen
- Clinical Conditions of Hepatitis BDokument2 SeitenClinical Conditions of Hepatitis BnurseNoch keine Bewertungen
- Nejm 2016:374:562Dokument9 SeitenNejm 2016:374:562Piya TangNoch keine Bewertungen
- Gary Null Anti-Aging Protocol For Nursing Homes - StudiesDokument748 SeitenGary Null Anti-Aging Protocol For Nursing Homes - StudiesEmre GunduzNoch keine Bewertungen
- Part C - Multiple SclerosisDokument4 SeitenPart C - Multiple SclerosisStaph AureusNoch keine Bewertungen
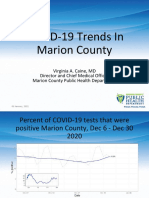
- Marion County Public Health Update 01.07.21Dokument15 SeitenMarion County Public Health Update 01.07.21Last DayNoch keine Bewertungen
- Systemic MycosisDokument15 SeitenSystemic Mycosisapi-19969058Noch keine Bewertungen
- Median Rhomboid GlossitisDokument4 SeitenMedian Rhomboid GlossitisYeltserNoch keine Bewertungen
- Licensing Manual PCH 082813Dokument32 SeitenLicensing Manual PCH 082813dikivNoch keine Bewertungen
- About Monkey PoxDokument3 SeitenAbout Monkey PoxObakoma Josiah100% (1)