Das könnte Ihnen auch gefallen
- PNF Techniques for Strengthening MusclesDokument76 SeitenPNF Techniques for Strengthening MusclesHasan KhawaldehNoch keine Bewertungen
- The Fundamentals of PNFDokument5 SeitenThe Fundamentals of PNFAri SudarsonoNoch keine Bewertungen
- ROM and manual stretching worksheetDokument12 SeitenROM and manual stretching worksheetMike ConnorsNoch keine Bewertungen
- Post Stroke Functional Exercises For RehabilitationDokument37 SeitenPost Stroke Functional Exercises For Rehabilitationjoel_simon_23100% (1)
- Orthopedic Physiotherapy Assignment: 1. Patient HistoryDokument4 SeitenOrthopedic Physiotherapy Assignment: 1. Patient HistoryarushiNoch keine Bewertungen
- Range of Motion and Mobility ExercisesDokument64 SeitenRange of Motion and Mobility ExercisesMae Arra Gilbao Lecobu-anNoch keine Bewertungen
- Glassgow Coma Scale and Rancho Los AmigosDokument17 SeitenGlassgow Coma Scale and Rancho Los AmigosHEMA CHANDRANNoch keine Bewertungen
- Brunnstrom ApproachDokument33 SeitenBrunnstrom ApproachAISHWARYA SWAMINATHANNoch keine Bewertungen
- B P O M: Rachial Lexus Utcome EasureDokument14 SeitenB P O M: Rachial Lexus Utcome EasureVirginia Feren FraganzhaNoch keine Bewertungen
- Gait in Children With Cerebral PalsyDokument5 SeitenGait in Children With Cerebral PalsyvarahamihirNoch keine Bewertungen
- ApproachDokument37 SeitenApproachAshu AshNoch keine Bewertungen
- Case History Frozen ShoulderDokument2 SeitenCase History Frozen ShoulderSaliha Akram0% (1)
- Neurological Assessment in the First Two Years of LifeVon EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniNoch keine Bewertungen
- Gait PatternsDokument2 SeitenGait Patternsandy123_appNoch keine Bewertungen
- Berg Balance ScaleDokument4 SeitenBerg Balance ScaleSanjanaNoch keine Bewertungen
- Movement Disorders Types - Mayo ClinicDokument1 SeiteMovement Disorders Types - Mayo ClinicdrrajmptnNoch keine Bewertungen
- Functional Re-EducationDokument8 SeitenFunctional Re-EducationPratibha SalkarNoch keine Bewertungen
- Active Movements Active Movements: By: DR - Chaman LalDokument51 SeitenActive Movements Active Movements: By: DR - Chaman LalAmbreena RasoolNoch keine Bewertungen
- Rood Approach Muscle RehabilitationDokument33 SeitenRood Approach Muscle RehabilitationCedricFernandez100% (1)
- Mirror Box Presentation Handout EditedDokument4 SeitenMirror Box Presentation Handout Editedapi-364398898Noch keine Bewertungen
- ACL Reconstruction Rehab in Soccer PlayerDokument8 SeitenACL Reconstruction Rehab in Soccer PlayerLidia DebbyNoch keine Bewertungen
- 2012 Mirror Therapy For Improving Motor Function After StrokeDokument68 Seiten2012 Mirror Therapy For Improving Motor Function After StrokeMarcelo Ortiz Valenzuela100% (1)
- Shoulder Impingement GuidelinesDokument3 SeitenShoulder Impingement GuidelinesTasha MillerNoch keine Bewertungen
- Muscle Grading and Testing ProceduresDokument5 SeitenMuscle Grading and Testing Proceduresshodhganga100% (1)
- Neurological ExaminationDokument13 SeitenNeurological Examinationsaveetha purushothamanNoch keine Bewertungen
- Bells Palsy Physio PDFDokument71 SeitenBells Palsy Physio PDFडा. सत्यदेव त्यागी आर्यNoch keine Bewertungen
- AOPA Handout NewParadigms Sciences IMPDokument34 SeitenAOPA Handout NewParadigms Sciences IMPAnup PednekarNoch keine Bewertungen
- Disability Evaluation: Radhika ChintamaniDokument58 SeitenDisability Evaluation: Radhika ChintamaniBhavya Amin0% (1)
- Physiotherapy management of paediatric flat feetDokument20 SeitenPhysiotherapy management of paediatric flat feetCalvina Mizumi100% (1)
- Therapeutic Exercise: Impact on Physical FunctionDokument30 SeitenTherapeutic Exercise: Impact on Physical FunctionMyrgen TingsonNoch keine Bewertungen
- Examine Cervical Spine Range MotionDokument16 SeitenExamine Cervical Spine Range MotionlecturioNoch keine Bewertungen
- Manual Muscle Testing of Infants, Toddlers, & Preschool ChildrenDokument7 SeitenManual Muscle Testing of Infants, Toddlers, & Preschool Childrendeasy100% (1)
- Range of Motion Chart EvaluationDokument2 SeitenRange of Motion Chart Evaluationtomeytto100% (1)
- Power Work and Energy Sport BiomechanicsDokument23 SeitenPower Work and Energy Sport BiomechanicsJosh KoenNoch keine Bewertungen
- Antenatal and Postnatal PPT PDFDokument15 SeitenAntenatal and Postnatal PPT PDFNikita -0251 ENoch keine Bewertungen
- KMC Dept of Orthopaedics Floor Reaction OrthosisDokument5 SeitenKMC Dept of Orthopaedics Floor Reaction OrthosischinmayghaisasNoch keine Bewertungen
- Endocrine Response Ni FinalDokument35 SeitenEndocrine Response Ni FinalSaktriawan ArifNoch keine Bewertungen
- FIM Score Sheet1Dokument2 SeitenFIM Score Sheet1Devasya0% (1)
- Design of A Hand OrthosisDokument251 SeitenDesign of A Hand OrthosisIsrael BlancoNoch keine Bewertungen
- Cardio Pulmonary AssessmentDokument8 SeitenCardio Pulmonary AssessmentSHAIK SHABEENANoch keine Bewertungen
- Effect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly PopulationDokument6 SeitenEffect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly Populationastrinila fauziNoch keine Bewertungen
- Cayuga Medical Center Pediatric Therapy ProgramDokument2 SeitenCayuga Medical Center Pediatric Therapy ProgramMhmd IrakyNoch keine Bewertungen
- Jurnal Frozen ShoulderDokument21 SeitenJurnal Frozen ShoulderMega Mulya Dwi FitriyaniNoch keine Bewertungen
- FIM or WeeFIM Assessment Scoresheet 2020Dokument3 SeitenFIM or WeeFIM Assessment Scoresheet 2020Mayco BiasibettiNoch keine Bewertungen
- Rehabilitation in Spinal Cord InjuryDokument2 SeitenRehabilitation in Spinal Cord InjuryAudry ArifinNoch keine Bewertungen
- Leg and Ankle Problems in Primary Care: Briant W. Smith, MD Orthopedic Surgery TPMGDokument50 SeitenLeg and Ankle Problems in Primary Care: Briant W. Smith, MD Orthopedic Surgery TPMGArmiya RamliNoch keine Bewertungen
- Active Movements: Dr:Maryam Memon Lecturer: JmiprsDokument33 SeitenActive Movements: Dr:Maryam Memon Lecturer: JmiprsAazeen memonNoch keine Bewertungen
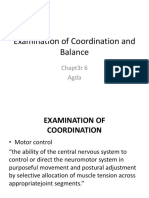
- Examination of Coordination and BalanceDokument27 SeitenExamination of Coordination and BalanceBelle AgdaNoch keine Bewertungen
- Energy conservation techniques for respiratory patientsDokument9 SeitenEnergy conservation techniques for respiratory patientsqwas zNoch keine Bewertungen
- Motor Learning Theory: References: Cole & Tufano, Chapter 19 Reserve Article: Mathiowetz & Bass Haugen (1994) AJOTDokument27 SeitenMotor Learning Theory: References: Cole & Tufano, Chapter 19 Reserve Article: Mathiowetz & Bass Haugen (1994) AJOTSundar SweeNoch keine Bewertungen
- Pilates Exercises (Inglés) (Artículo) - Salvi ShahDokument8 SeitenPilates Exercises (Inglés) (Artículo) - Salvi ShahJose Luis Ramos MolloNoch keine Bewertungen
- Motor Control TheoriesDokument94 SeitenMotor Control TheoriesAhmad Dur IhsanNoch keine Bewertungen
- ICUDokument12 SeitenICUNabilahNoch keine Bewertungen
- Balance TestDokument21 SeitenBalance TestSyazaWajihahZulkefliNoch keine Bewertungen
- The Learning Process: Definition and Perspective of LearningDokument40 SeitenThe Learning Process: Definition and Perspective of LearningMarjorie Ventuales Libo-onNoch keine Bewertungen
- SCALE-Selective Control Assesment PDFDokument3 SeitenSCALE-Selective Control Assesment PDFjinil raj j.r.Noch keine Bewertungen
- Chest Physical Therapy by Abdul Ghafoor Sajjad AFIRMDokument4 SeitenChest Physical Therapy by Abdul Ghafoor Sajjad AFIRMAbdul Ghafoor SajjadNoch keine Bewertungen
- Pilates InserviceDokument11 SeitenPilates InserviceToni MansfieldNoch keine Bewertungen
- PNF FullDokument46 SeitenPNF FullHUZAIFA YAMAAN100% (1)
- PT ResumeDokument2 SeitenPT Resumeapi-518034073Noch keine Bewertungen
- PT Cover LetterDokument1 SeitePT Cover Letterapi-518034073Noch keine Bewertungen
- Scholarly Project FinalDokument46 SeitenScholarly Project Finalapi-518034073Noch keine Bewertungen
- Professional Behaviors 2Dokument13 SeitenProfessional Behaviors 2api-518034073Noch keine Bewertungen
- Chronic Pain CertDokument1 SeiteChronic Pain Certapi-518034073Noch keine Bewertungen
- Massive RTC Case PresentationDokument24 SeitenMassive RTC Case Presentationapi-518034073Noch keine Bewertungen
- Inservice Multiple Myeloma and Physical RehabilitationDokument3 SeitenInservice Multiple Myeloma and Physical Rehabilitationapi-518034073Noch keine Bewertungen
- Industrial ProjectDokument39 SeitenIndustrial Projectapi-518034073Noch keine Bewertungen
- Documentation Continuing Education CertificateDokument1 SeiteDocumentation Continuing Education Certificateapi-518034073Noch keine Bewertungen
- Job Satisfaction RRLDokument39 SeitenJob Satisfaction RRLMarie Tiffany100% (1)
- Đề Thi Thử THPT 2021 - Tiếng Anh - GV Vũ Thị Mai Phương - Đề 13 - Có Lời GiảiDokument17 SeitenĐề Thi Thử THPT 2021 - Tiếng Anh - GV Vũ Thị Mai Phương - Đề 13 - Có Lời GiảiHanh YenNoch keine Bewertungen
- fLOW CHART FOR WORKER'S ENTRYDokument2 SeitenfLOW CHART FOR WORKER'S ENTRYshamshad ahamedNoch keine Bewertungen
- Infinite & Finite Slope1Dokument38 SeitenInfinite & Finite Slope1CHUKKALA LEELA RAVALINoch keine Bewertungen
- Mabuhay Wedding Package2006Dokument3 SeitenMabuhay Wedding Package2006Darwin Dionisio ClementeNoch keine Bewertungen
- Haematology Notes - 3rd EdDokument100 SeitenHaematology Notes - 3rd EdSally Brit100% (1)
- WSO 2022 IB Working Conditions SurveyDokument42 SeitenWSO 2022 IB Working Conditions SurveyPhạm Hồng HuếNoch keine Bewertungen
- Analysis of Heavy Metals Concentration in Landfill Soil IJERTV8IS120019Dokument2 SeitenAnalysis of Heavy Metals Concentration in Landfill Soil IJERTV8IS120019Eustache NIJEJENoch keine Bewertungen
- Tumors of The Central Nervous System - VOL 12Dokument412 SeitenTumors of The Central Nervous System - VOL 12vitoNoch keine Bewertungen
- Practice of Epidemiology Performance of Floating Absolute RisksDokument4 SeitenPractice of Epidemiology Performance of Floating Absolute RisksShreyaswi M KarthikNoch keine Bewertungen
- PERSONS Finals Reviewer Chi 0809Dokument153 SeitenPERSONS Finals Reviewer Chi 0809Erika Angela GalceranNoch keine Bewertungen
- Business Startup Practical Plan PDFDokument70 SeitenBusiness Startup Practical Plan PDFShaji Viswanathan. Mcom, MBA (U.K)Noch keine Bewertungen
- Fluid Mechanics Sessional: Dhaka University of Engineering & Technology, GazipurDokument17 SeitenFluid Mechanics Sessional: Dhaka University of Engineering & Technology, GazipurMd saydul islamNoch keine Bewertungen
- Space Analysis in Orthodontic: University of GlasgowDokument16 SeitenSpace Analysis in Orthodontic: University of GlasgowNizam Muhamad100% (1)
- LabyrinthDokument4 SeitenLabyrinthAyezaZuberyNoch keine Bewertungen
- Switzerland: Food and CultureDokument18 SeitenSwitzerland: Food and CultureAaron CoutinhoNoch keine Bewertungen
- Lesson 1 CA 3Dokument13 SeitenLesson 1 CA 3myndleNoch keine Bewertungen
- Notice: Use of Segways® and Similar Devices by Individuals With A Mobility Impairment in GSA-Controlled Federal FacilitiesDokument2 SeitenNotice: Use of Segways® and Similar Devices by Individuals With A Mobility Impairment in GSA-Controlled Federal FacilitiesJustia.comNoch keine Bewertungen
- Very Easy Toeic Units 7 - 12 (Q1)Dokument39 SeitenVery Easy Toeic Units 7 - 12 (Q1)Minh KhaiNoch keine Bewertungen
- Pictorial History of AOTADokument5 SeitenPictorial History of AOTAThe American Occupational Therapy Association0% (4)
- Magnetic FieldDokument19 SeitenMagnetic FieldNitinSrivastava100% (2)
- EcR - 1 Leading and Lagging IndicatorsDokument10 SeitenEcR - 1 Leading and Lagging IndicatorsMiloš ĐukićNoch keine Bewertungen
- Human Capital FormationDokument9 SeitenHuman Capital Formationtannu singh67% (6)
- Philippines implements external quality assessment for clinical labsDokument2 SeitenPhilippines implements external quality assessment for clinical labsKimberly PeranteNoch keine Bewertungen
- Chemical and Physical Properties of Refined Petroleum ProductsDokument36 SeitenChemical and Physical Properties of Refined Petroleum Productskanakarao1Noch keine Bewertungen
- Nursing Diagnosis TemplateDokument6 SeitenNursing Diagnosis Templatesdk6972Noch keine Bewertungen
- Life Overseas 7 ThesisDokument20 SeitenLife Overseas 7 ThesisRene Jr MalangNoch keine Bewertungen
- December - Cost of Goods Sold (Journal)Dokument14 SeitenDecember - Cost of Goods Sold (Journal)kuro hanabusaNoch keine Bewertungen
- Retail Management PPT1Dokument14 SeitenRetail Management PPT1Srilekha GubbalaNoch keine Bewertungen
- Funds Flow Statement ExplainedDokument76 SeitenFunds Flow Statement Explainedthella deva prasad0% (1)