Das könnte Ihnen auch gefallen
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesVon EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesNoch keine Bewertungen
- Emergencies in Diabetes: Zulfachmi WahabDokument33 SeitenEmergencies in Diabetes: Zulfachmi WahablidawatiNoch keine Bewertungen
- Causes of An Elevated Serum Lactate Dehydrogenase LevelDokument3 SeitenCauses of An Elevated Serum Lactate Dehydrogenase LevelSantiago IllarramendiNoch keine Bewertungen
- Neurology MnemonicsDokument11 SeitenNeurology MnemonicsOstaz100% (1)
- Geriatric SyndromeDokument49 SeitenGeriatric Syndromewita prabawatiNoch keine Bewertungen
- Depressive Disorders - Psychiatric Disorders - MSD Manual Professional Edition.Dokument2 SeitenDepressive Disorders - Psychiatric Disorders - MSD Manual Professional Edition.Dragutin PetrićNoch keine Bewertungen
- Aula Diagnosis and Treatment of Primary Adrenal Insufficiency (Dokument25 SeitenAula Diagnosis and Treatment of Primary Adrenal Insufficiency (Bibiana Prada de Camargo ColenciNoch keine Bewertungen
- DeliriumDokument40 SeitenDeliriumAklile TsegaNoch keine Bewertungen
- Nursing Care of Patient With DementiaDokument23 SeitenNursing Care of Patient With DementiaRufus Raj100% (4)
- Adrenal CrisisDokument12 SeitenAdrenal CrisisShreyNoch keine Bewertungen
- Pemicu 1: Yinvill 405120025 Kelompok 8Dokument99 SeitenPemicu 1: Yinvill 405120025 Kelompok 8yinvilllNoch keine Bewertungen
- Table 25-8Dokument1 SeiteTable 25-8Dragutin PetrićNoch keine Bewertungen
- Table 25-8Dokument1 SeiteTable 25-8Dragutin PetrićNoch keine Bewertungen
- 10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureDokument119 Seiten10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureRanjit SharmaNoch keine Bewertungen
- Approach To Unconscious ChildDokument52 SeitenApproach To Unconscious Childar bindraNoch keine Bewertungen
- Confusion MetabolicDokument43 SeitenConfusion MetabolicYoumna ShaabanNoch keine Bewertungen
- Electrolyte Imbalances.: Mohamed Umer Amoud School of MedicineDokument23 SeitenElectrolyte Imbalances.: Mohamed Umer Amoud School of MedicineAbdisalan hassanNoch keine Bewertungen
- Penanganan Krisis HipertensiDokument36 SeitenPenanganan Krisis Hipertensisuho exoNoch keine Bewertungen
- Brain OdemaDokument2 SeitenBrain OdemaMohamed Nasreldin HamdoonNoch keine Bewertungen
- Approach To Comatose Child: DR G.VenkateshDokument83 SeitenApproach To Comatose Child: DR G.VenkateshG VenkateshNoch keine Bewertungen
- Seizures and EpilepsyDokument64 SeitenSeizures and EpilepsyrajaeasNoch keine Bewertungen
- Delirium, Dementia, PsychosisDokument2 SeitenDelirium, Dementia, PsychosisLagente EstalocaNoch keine Bewertungen
- Metabolic EncephalopathyDokument22 SeitenMetabolic Encephalopathytricia isabellaNoch keine Bewertungen
- Acute Chronic ComplicationDokument49 SeitenAcute Chronic ComplicationMuhammad DaviqNoch keine Bewertungen
- CASE StudyDokument5 SeitenCASE StudyMary Shane Aragon MoraldeNoch keine Bewertungen
- CardiomyopathyDokument8 SeitenCardiomyopathyKarisaNoch keine Bewertungen
- Syndrome of Inappropriate AdhDokument5 SeitenSyndrome of Inappropriate AdhCarloRafaelNoch keine Bewertungen
- HT Emergency Final DR Rinelia Minaswary, SPJPDokument46 SeitenHT Emergency Final DR Rinelia Minaswary, SPJPAfdhal MuhammadNoch keine Bewertungen
- Medical Complications of Alcohol Use: Moderator: DR Spoorthy Presenter: DR NeethuDokument45 SeitenMedical Complications of Alcohol Use: Moderator: DR Spoorthy Presenter: DR NeethuSensibleNoch keine Bewertungen
- Drug StudyDokument6 SeitenDrug Studyi_existNoch keine Bewertungen
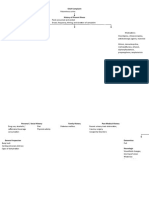
- conceptmap-DIABETES MELLITUSDokument8 Seitenconceptmap-DIABETES MELLITUSDonnabell DayudayNoch keine Bewertungen
- Albalos - Drug StudyDokument1 SeiteAlbalos - Drug StudyMia GarciaNoch keine Bewertungen
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDokument92 SeitenHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoNoch keine Bewertungen
- DR Rukma Cardio Cardiovascular EmergencyDokument31 SeitenDR Rukma Cardio Cardiovascular EmergencyAmanda DavisNoch keine Bewertungen
- Hipertensi EmergencyDokument31 SeitenHipertensi Emergencysar tikaNoch keine Bewertungen
- Pa 02 CardioDokument45 SeitenPa 02 CardioElly NuñezNoch keine Bewertungen
- Dementia Recentupdates 130920080812 Phpapp01Dokument58 SeitenDementia Recentupdates 130920080812 Phpapp01SantanuNoch keine Bewertungen
- The Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MDokument51 SeitenThe Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MYohanna SinuhajiNoch keine Bewertungen
- Altered Mental StateDokument2 SeitenAltered Mental Stateizzati94Noch keine Bewertungen
- Chemical & Drug InjuriesDokument23 SeitenChemical & Drug Injuriesjulo_05Noch keine Bewertungen
- Iskemia Kerusakan Membran Nekrosis Sel Gangguan Sel Ca InflukDokument12 SeitenIskemia Kerusakan Membran Nekrosis Sel Gangguan Sel Ca Influkmuhammad_aulia_5Noch keine Bewertungen
- Neuropsychological Assessment of DementiaDokument44 SeitenNeuropsychological Assessment of DementiaAdam Mochtar100% (1)
- SyncopeDokument67 SeitenSyncopenosloba31Noch keine Bewertungen
- Introduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Dokument2 SeitenIntroduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Nikki VillanuevaNoch keine Bewertungen
- Nursing Care of Stroke - NewDokument4 SeitenNursing Care of Stroke - Newninda saputriNoch keine Bewertungen
- Epilepsy: Dr. Fitriyani SP.SDokument31 SeitenEpilepsy: Dr. Fitriyani SP.Skurnia saptaNoch keine Bewertungen
- PolyuriaDokument5 SeitenPolyuriaKrisha Marie BadilloNoch keine Bewertungen
- DELIRIUMDokument68 SeitenDELIRIUMVarada PanikkathNoch keine Bewertungen
- CKD - Hema, Endo, Neuro, Derma Aspects - JAMESDokument163 SeitenCKD - Hema, Endo, Neuro, Derma Aspects - JAMESJosephinerose CaraveoNoch keine Bewertungen
- 20) Dr. Dr. Himawan Sanusi, Sp. PD, KEMD - Cushing+conn+addsosnianDokument27 Seiten20) Dr. Dr. Himawan Sanusi, Sp. PD, KEMD - Cushing+conn+addsosnianAsridewi DewiNoch keine Bewertungen
- CPC Medical Oncology 2Dokument52 SeitenCPC Medical Oncology 2Ravi KumarNoch keine Bewertungen
- Bowley Neuropathy Plexopathy Radiculopathy 2022Dokument58 SeitenBowley Neuropathy Plexopathy Radiculopathy 2022Hassan IbrahimNoch keine Bewertungen
- Unit 3Dokument21 SeitenUnit 3dekNoch keine Bewertungen
- Neurological Emergencies d10Dokument60 SeitenNeurological Emergencies d10Diana NurulNoch keine Bewertungen
- Environmental Pathology: Chemical & Drug Injuries: Ma. Minda Luz M. Manuguid, M.DDokument22 SeitenEnvironmental Pathology: Chemical & Drug Injuries: Ma. Minda Luz M. Manuguid, M.Djulo_05Noch keine Bewertungen
- Thyroid Gland Clin PathDokument2 SeitenThyroid Gland Clin PathIanMayNoch keine Bewertungen
- Toxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiDokument18 SeitenToxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiVivi DeviyanaNoch keine Bewertungen
- Cardiac EmergenciesDokument18 SeitenCardiac EmergenciesJoice DasNoch keine Bewertungen
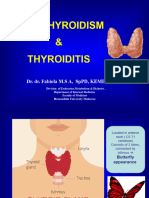
- Hipotiroid Dan Tiroiditis 2023Dokument53 SeitenHipotiroid Dan Tiroiditis 2023ramadhanadlansyah7Noch keine Bewertungen
- Carol Rivers'board Review FlashcardsDokument440 SeitenCarol Rivers'board Review FlashcardsJennelle CadoganNoch keine Bewertungen
- Ophthalmology-Development of EyeDokument20 SeitenOphthalmology-Development of EyeRahul Kumar DiwakarNoch keine Bewertungen
- Postpartum Blues: by DR Wangari KuriaDokument9 SeitenPostpartum Blues: by DR Wangari KuriaRahul Kumar DiwakarNoch keine Bewertungen
- ENT-Laryngeal ParalysisDokument26 SeitenENT-Laryngeal ParalysisRahul Kumar DiwakarNoch keine Bewertungen
- OBS & Gynec-Antepartum HaemorrhageDokument18 SeitenOBS & Gynec-Antepartum HaemorrhageRahul Kumar DiwakarNoch keine Bewertungen
- Ward 8M: Evaluation of Thought Process and SpeechDokument17 SeitenWard 8M: Evaluation of Thought Process and SpeechRahul Kumar DiwakarNoch keine Bewertungen
- Intellectual Disability/ Mental Retardation: Level IV Tutorial 2015/2016 DR J. KamauDokument21 SeitenIntellectual Disability/ Mental Retardation: Level IV Tutorial 2015/2016 DR J. KamauRahul Kumar DiwakarNoch keine Bewertungen
- Psychological Aspects of HIVDokument17 SeitenPsychological Aspects of HIVRahul Kumar DiwakarNoch keine Bewertungen
- Delirium: by Pius KigamwaDokument15 SeitenDelirium: by Pius KigamwaRahul Kumar DiwakarNoch keine Bewertungen
- Antidepressants PrintedDokument3 SeitenAntidepressants PrintedRahul Kumar DiwakarNoch keine Bewertungen
- Human Devlopment 1: Level 1Dokument27 SeitenHuman Devlopment 1: Level 1Rahul Kumar DiwakarNoch keine Bewertungen
- Pain and Behavior: Objectives - Understand Purpose of Pain - Pain Pathway - Differences On Different IndividualsDokument26 SeitenPain and Behavior: Objectives - Understand Purpose of Pain - Pain Pathway - Differences On Different IndividualsRahul Kumar DiwakarNoch keine Bewertungen
- HELPPP FinalDokument55 SeitenHELPPP FinalRahul Kumar DiwakarNoch keine Bewertungen
- Training Guide: Recording and Handling of Schedule 8 Drugs in Hospital WardsDokument41 SeitenTraining Guide: Recording and Handling of Schedule 8 Drugs in Hospital WardsRahul Kumar DiwakarNoch keine Bewertungen
- Emergency Psychiatry: SuicideDokument3 SeitenEmergency Psychiatry: SuicideRahul Kumar Diwakar100% (1)
- Eating Disorders: by Pius KigamwaDokument20 SeitenEating Disorders: by Pius KigamwaRahul Kumar DiwakarNoch keine Bewertungen
- Group Work Case Study Problems-1Dokument7 SeitenGroup Work Case Study Problems-1Rahul Kumar DiwakarNoch keine Bewertungen
- Male Sexual Disordees: Tutorial Level 4-2015Dokument57 SeitenMale Sexual Disordees: Tutorial Level 4-2015Rahul Kumar DiwakarNoch keine Bewertungen
- SUBSTANCE ABUSEpresentation Level 4Dokument43 SeitenSUBSTANCE ABUSEpresentation Level 4Rahul Kumar Diwakar100% (1)
- Schizophrenia and Other Psychotic Disorders: DR Rachel Kang'Ethe Department of PsychiatryDokument76 SeitenSchizophrenia and Other Psychotic Disorders: DR Rachel Kang'Ethe Department of PsychiatryRahul Kumar Diwakar100% (1)
- Process of Rehabilitation in PsychiatryDokument29 SeitenProcess of Rehabilitation in PsychiatryRahul Kumar DiwakarNoch keine Bewertungen
- What You Should Know About COVID-19 To Protect Yourself and OthersDokument2 SeitenWhat You Should Know About COVID-19 To Protect Yourself and OthersRahul Kumar DiwakarNoch keine Bewertungen
- Lesson Plan DepressionDokument19 SeitenLesson Plan DepressionRahul Kumar Diwakar100% (1)
- Schizophrenia Lecture 2010 PART 1 and 2Dokument69 SeitenSchizophrenia Lecture 2010 PART 1 and 2Rahul Kumar DiwakarNoch keine Bewertungen
- Drug Addiction: Alcohol Other Substances Counselling Class Lesson 6Dokument34 SeitenDrug Addiction: Alcohol Other Substances Counselling Class Lesson 6Rahul Kumar DiwakarNoch keine Bewertungen
- Psychological Aspects of HIV-level IIDokument18 SeitenPsychological Aspects of HIV-level IIRahul Kumar DiwakarNoch keine Bewertungen
- Review Artilces Annals and Essences of DentistryDokument14 SeitenReview Artilces Annals and Essences of DentistryRahul Kumar DiwakarNoch keine Bewertungen
- AtharvasheershamDokument5 SeitenAtharvasheershamforthegroupsNoch keine Bewertungen
- Catalogue Mega EnglishDokument40 SeitenCatalogue Mega EnglishInotech Outillage Nouvelle CalédonieNoch keine Bewertungen
- QAS M001 SLPS Quality Assurance ManualDokument49 SeitenQAS M001 SLPS Quality Assurance ManualMHDNoch keine Bewertungen
- October 2014 1413376166 06 PDFDokument3 SeitenOctober 2014 1413376166 06 PDFDineshNoch keine Bewertungen
- MAPEH 1 (4th Quarter)Dokument27 SeitenMAPEH 1 (4th Quarter)JESSELLY VALESNoch keine Bewertungen
- PP Planning Workshop SAPDokument36 SeitenPP Planning Workshop SAPDavid100% (1)
- Soil MechDokument21 SeitenSoil MechAhsan AbbasNoch keine Bewertungen
- Crim 2 Module 2 Atty A.D.G.Dokument7 SeitenCrim 2 Module 2 Atty A.D.G.Badens DgNoch keine Bewertungen
- Qualitative Analysis of Selected Medicinal Plants, Tamilnadu, IndiaDokument3 SeitenQualitative Analysis of Selected Medicinal Plants, Tamilnadu, IndiaDiana RaieNoch keine Bewertungen
- Alcatel 9400 PDFDokument4 SeitenAlcatel 9400 PDFNdambuki DicksonNoch keine Bewertungen
- The Biography of Hazrat Shah Qamaos Sahib in One PageDokument3 SeitenThe Biography of Hazrat Shah Qamaos Sahib in One PageMohammed Abdul Hafeez, B.Com., Hyderabad, IndiaNoch keine Bewertungen
- Engineering Discourse Communities RMDokument4 SeitenEngineering Discourse Communities RMapi-336463296Noch keine Bewertungen
- Fractal Blaster Trading Strategy ReportDokument22 SeitenFractal Blaster Trading Strategy ReportIcky IckyNoch keine Bewertungen
- F22 RaptorDokument2 SeitenF22 RaptorKakhaNoch keine Bewertungen
- Exercise No. 2 (DCC First and Second Summary)Dokument3 SeitenExercise No. 2 (DCC First and Second Summary)Lalin-Mema LRNoch keine Bewertungen
- Celebrations Around The WorldDokument3 SeitenCelebrations Around The WorldpaolaNoch keine Bewertungen
- Airplus CDF3 Technical SpecsDokument38 SeitenAirplus CDF3 Technical Specssadik FreelancerNoch keine Bewertungen
- Alberico Da BarbianoDokument3 SeitenAlberico Da BarbianoNupur PalNoch keine Bewertungen
- Vmware Virtualization Health Check ServiceDokument13 SeitenVmware Virtualization Health Check ServicetvuongphamNoch keine Bewertungen
- Allama Iqbal Open University, Islamabad: (Secondary Teacher Education Department) WarningDokument2 SeitenAllama Iqbal Open University, Islamabad: (Secondary Teacher Education Department) WarningAiNa KhanNoch keine Bewertungen
- Wipro Home Office RangeDokument8 SeitenWipro Home Office RangePrashant RawatNoch keine Bewertungen
- Finance Budget - Ankur WarikooDokument28 SeitenFinance Budget - Ankur WarikooVivek Gupta100% (1)
- AutoPIPE Tutorial PDFDokument156 SeitenAutoPIPE Tutorial PDFdhaktodesatyajitNoch keine Bewertungen
- Program 2019 MTAPTL Annual Convention PDFDokument3 SeitenProgram 2019 MTAPTL Annual Convention PDFrichardlfigueroaNoch keine Bewertungen
- Glide Reflection Folding InstructionsDokument1 SeiteGlide Reflection Folding Instructionsapi-355107616Noch keine Bewertungen
- Price and Output Determination Under OligopolyDokument26 SeitenPrice and Output Determination Under OligopolySangitha Nadar100% (1)
- Digital Dash I/O Adapter Configuration: Connector Pin FunctionsDokument8 SeitenDigital Dash I/O Adapter Configuration: Connector Pin FunctionsAfeef Ibn AlbraNoch keine Bewertungen
- Job Board Week WhituDokument5 SeitenJob Board Week WhituAnonymous MZh1KUUXNoch keine Bewertungen
- Creative Thesis ExamplesDokument8 SeitenCreative Thesis Examplescatherinebitkerrochester100% (2)
- Dialogue-2: Problem of Our CountryDokument6 SeitenDialogue-2: Problem of Our CountrysiamNoch keine Bewertungen