Das könnte Ihnen auch gefallen
- Nursing AuditDokument26 SeitenNursing AuditJoe ShewaleNoch keine Bewertungen
- Nursing AuditDokument3 SeitenNursing AuditJoe Shewale0% (1)
- Nursing AuditDokument36 SeitenNursing AuditPhebeDimpleNoch keine Bewertungen
- Patient Assignment MethodDokument48 SeitenPatient Assignment Methodsathya Arunkumar100% (1)
- Aa Developing Staffing PatternsDokument14 SeitenAa Developing Staffing PatternsAkshata BansodeNoch keine Bewertungen
- Patient Assignmen PresentationtDokument12 SeitenPatient Assignmen PresentationtSuraj Raj SubediNoch keine Bewertungen
- Nightingale Institute of Nursing, Noida: Equipment UtilizationDokument13 SeitenNightingale Institute of Nursing, Noida: Equipment UtilizationDhAiRyA ArOrANoch keine Bewertungen
- Quality CareDokument7 SeitenQuality CareOpeyemi OmolabakeNoch keine Bewertungen
- Essentials of Nursing Educational InstitutionDokument11 SeitenEssentials of Nursing Educational InstitutionLuke ShantiNoch keine Bewertungen
- MiesDokument40 SeitenMiessanthiyasandyNoch keine Bewertungen
- Performance Appraisal For Nursing PersonnelDokument9 SeitenPerformance Appraisal For Nursing PersonnelJoel Vi PriNoch keine Bewertungen
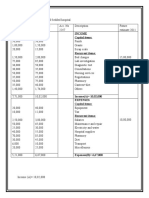
- Income Capital ItemsDokument2 SeitenIncome Capital ItemsDeepti KukretiNoch keine Bewertungen
- Con Mission, Vision, ObjectivesDokument1 SeiteCon Mission, Vision, ObjectivesMelchor Felipe SalvosaNoch keine Bewertungen
- Pioneer Nursing College, Vadodar A:: Nursing Management: Pert, Mbo, Gantt ChartDokument45 SeitenPioneer Nursing College, Vadodar A:: Nursing Management: Pert, Mbo, Gantt ChartKinjal VasavaNoch keine Bewertungen
- PertDokument34 SeitenPertVikrant ChaudharyNoch keine Bewertungen
- Problems of Speciality Unit and Their Solution - 041536Dokument7 SeitenProblems of Speciality Unit and Their Solution - 041536Shubhrima KhanNoch keine Bewertungen
- Cont EduDokument18 SeitenCont EduShilu Mathai PappachanNoch keine Bewertungen
- Paper PresentationDokument5 SeitenPaper PresentationSamjaisheel SamsonNoch keine Bewertungen
- Fiscalplanning Sanil 131223005213 Phpapp01Dokument44 SeitenFiscalplanning Sanil 131223005213 Phpapp01San Miguel SouthNoch keine Bewertungen
- Evaluationppt 110926211536 Phpapp01Dokument35 SeitenEvaluationppt 110926211536 Phpapp01Seema VashishtNoch keine Bewertungen
- A Case of Sheehan's Syndrome: A Rare But Life - Threatening ComplicationDokument2 SeitenA Case of Sheehan's Syndrome: A Rare But Life - Threatening ComplicationEditor IJTSRDNoch keine Bewertungen
- Presentation FPAI 2014 2Dokument20 SeitenPresentation FPAI 2014 2Sameer Dubey0% (1)
- Seminar Topic - Job Description of Departmental SisterDokument18 SeitenSeminar Topic - Job Description of Departmental Sistershubham rathod0% (1)
- First Referral UnitDokument24 SeitenFirst Referral Unitjay5ar5jamorabon5torNoch keine Bewertungen
- Professional Organization22Dokument19 SeitenProfessional Organization22ValarmathiNoch keine Bewertungen
- Health Care Delivery Concerns, National Health andDokument26 SeitenHealth Care Delivery Concerns, National Health andKavi rajputNoch keine Bewertungen
- Organisational Structure of HospitalDokument4 SeitenOrganisational Structure of HospitalNaveen EldoseNoch keine Bewertungen
- Roles and Responsibilitis of Community Health NurseDokument22 SeitenRoles and Responsibilitis of Community Health NurseAnusha AnishNoch keine Bewertungen
- CURRICULUM RESEARCH IN NURSING - WordDokument4 SeitenCURRICULUM RESEARCH IN NURSING - WordSMITHA JOSENoch keine Bewertungen
- Observation Visit To NSDokument12 SeitenObservation Visit To NSpriyaNoch keine Bewertungen
- Seminar Obgyn Chemotheraphy in GynaecologyDokument38 SeitenSeminar Obgyn Chemotheraphy in GynaecologyRoshandiep GillNoch keine Bewertungen
- Manager Behaviour andDokument11 SeitenManager Behaviour andsimmyvashishtNoch keine Bewertungen
- State Nurses Registration CouncilDokument2 SeitenState Nurses Registration CouncilGagan100% (3)
- Mission, Vision, Philosophy and ObjectivesDokument49 SeitenMission, Vision, Philosophy and ObjectivesNeethu JoseNoch keine Bewertungen
- RecruitmentDokument54 SeitenRecruitmentRam SankarNoch keine Bewertungen
- Staffing - Nursing, Staffing Norms, Staff Estimation and SchedulingDokument54 SeitenStaffing - Nursing, Staffing Norms, Staff Estimation and SchedulingSanjay Kumar SanjuNoch keine Bewertungen
- Duties and Responsibilities of Various Category of Nursing Personnel 12Dokument10 SeitenDuties and Responsibilities of Various Category of Nursing Personnel 12Anusikta Panda100% (1)
- Mobile Coronary Care UnitDokument16 SeitenMobile Coronary Care UnitArcha100% (2)
- Assam Nurses' Midwives' & Health Visitors' CouncilDokument2 SeitenAssam Nurses' Midwives' & Health Visitors' CouncilnafisnazarNoch keine Bewertungen
- Use of Computers in Teaching, Learning, Research & Nursing PracticeDokument24 SeitenUse of Computers in Teaching, Learning, Research & Nursing PracticeStephy SojanNoch keine Bewertungen
- By:-Firoz Qureshi Dept. Psychiatric NursingDokument46 SeitenBy:-Firoz Qureshi Dept. Psychiatric NursingrajeshwariNoch keine Bewertungen
- Kauvery Hospital:: Kauvery Medical Centre-2002 - KMC Speciality Hospital Has Named As Kauvery Hospital. 2004Dokument21 SeitenKauvery Hospital:: Kauvery Medical Centre-2002 - KMC Speciality Hospital Has Named As Kauvery Hospital. 2004Sashi Kumar0% (1)
- Budget PPTDokument15 SeitenBudget PPTbushraanwarNoch keine Bewertungen
- Role of Regulatoy/Statutory Bodies in Nursing: Ishrat A. Patel 1 Year MSC NursingDokument31 SeitenRole of Regulatoy/Statutory Bodies in Nursing: Ishrat A. Patel 1 Year MSC NursingIshrat PatelNoch keine Bewertungen
- Polio PgramDokument3 SeitenPolio PgramRenita Chris100% (2)
- NABH Staff RatioDokument1 SeiteNABH Staff RatioRetteri KUMARANNoch keine Bewertungen
- School Health Service: Dept. of Community MedicineDokument20 SeitenSchool Health Service: Dept. of Community MedicineAhsan Ul Kayum BhuiyanNoch keine Bewertungen
- FF Staff Relationship and TechniquesDokument15 SeitenFF Staff Relationship and TechniquesAnkita Patel100% (1)
- Evaluation Proforma For Case StudyDokument2 SeitenEvaluation Proforma For Case Studypriyanjali sainiNoch keine Bewertungen
- TNAIDokument11 SeitenTNAISimran Josan100% (1)
- Concept of Inservice EducationDokument4 SeitenConcept of Inservice EducationRoselineTigga100% (1)
- Health Care Deliver System in IndiaDokument13 SeitenHealth Care Deliver System in IndiaRinkal UpadhyayNoch keine Bewertungen
- Hospital Management Information SystemDokument22 SeitenHospital Management Information SystemLakshmi Rj100% (1)
- Legal Aspect of DocumentationDokument16 SeitenLegal Aspect of DocumentationabidNoch keine Bewertungen
- Guidelines For GNMDokument11 SeitenGuidelines For GNMJeya Rani100% (1)
- Maintenance of Supplies and EquipmentsDokument11 SeitenMaintenance of Supplies and EquipmentsCheranmadevi Padavettan100% (1)
- 1) Student Leave RecordDokument1 Seite1) Student Leave RecordMuhd Fakhrul HazimmNoch keine Bewertungen
- Identify The Problems of The Speciality Units To Develop Plan of Action by Using Problem Solving AppraoachDokument19 SeitenIdentify The Problems of The Speciality Units To Develop Plan of Action by Using Problem Solving Appraoachvani reddyNoch keine Bewertungen
- Management: Prepared By-Ms. Anshu M.Sc. Nursing 2 Year KGMU Institute of NursingDokument35 SeitenManagement: Prepared By-Ms. Anshu M.Sc. Nursing 2 Year KGMU Institute of NursingKapil VermaNoch keine Bewertungen
- History of Community Health and Community Health Nursing: Uma J Deaver Asst Professor MM College of NursingDokument46 SeitenHistory of Community Health and Community Health Nursing: Uma J Deaver Asst Professor MM College of NursingKapil VermaNoch keine Bewertungen
- Human Resource Management: Meenakshi Soni Lecturer College of Nursing, JaipurDokument18 SeitenHuman Resource Management: Meenakshi Soni Lecturer College of Nursing, JaipurKapil VermaNoch keine Bewertungen
- Control Valve FunctionDokument1 SeiteControl Valve FunctionKapil VermaNoch keine Bewertungen
- Pert Gantt Chart & MBO: Presesnted By: Navaneeta Kusum M.Sc. NSG 2 YRDokument31 SeitenPert Gantt Chart & MBO: Presesnted By: Navaneeta Kusum M.Sc. NSG 2 YRKapil VermaNoch keine Bewertungen
- Nursing AuditDokument29 SeitenNursing AuditKapil VermaNoch keine Bewertungen
- Bench Marking: Meenakshi Soni Lecturer College of Nursing, JaipurDokument11 SeitenBench Marking: Meenakshi Soni Lecturer College of Nursing, JaipurKapil VermaNoch keine Bewertungen
- 3-Axis Accelerometer and Processing - Robot Is HappyDokument4 Seiten3-Axis Accelerometer and Processing - Robot Is HappyKapil VermaNoch keine Bewertungen
- Marine Engineering PracticeDokument13 SeitenMarine Engineering PracticeKapil Verma100% (1)
- Address LionDokument16 SeitenAddress LionKapil VermaNoch keine Bewertungen
- Meo Oral AnsDokument17 SeitenMeo Oral AnsKapil Verma100% (4)
- Development of COMMUNITY HEALTH NURSING in IndiaDokument12 SeitenDevelopment of COMMUNITY HEALTH NURSING in IndiaKapil Verma100% (3)
- Amendments To The MARPOL Convention From 01 January 2013.: 1. BackgroundDokument10 SeitenAmendments To The MARPOL Convention From 01 January 2013.: 1. BackgroundKapil VermaNoch keine Bewertungen
- Assignment No:: ToolsDokument3 SeitenAssignment No:: ToolsKapil VermaNoch keine Bewertungen
- Propeller Cap TurbineDokument4 SeitenPropeller Cap TurbineKapil VermaNoch keine Bewertungen
- Mep Oral Questions in BulkDokument20 SeitenMep Oral Questions in BulkKapil Verma100% (1)
- Fluid Valve NotesDokument12 SeitenFluid Valve NotesKapil VermaNoch keine Bewertungen
- Pujangga Piping - The Meaning of Valves - Only The BasicDokument21 SeitenPujangga Piping - The Meaning of Valves - Only The BasicKapil VermaNoch keine Bewertungen
- Cylinder Relief Valve InformationDokument2 SeitenCylinder Relief Valve InformationKapil VermaNoch keine Bewertungen
- Ice-Breaking Activities For The 1st Day of SchoolDokument2 SeitenIce-Breaking Activities For The 1st Day of SchoolEssam SayedNoch keine Bewertungen
- Chapter 4 Emp InvolvementDokument9 SeitenChapter 4 Emp InvolvementVikram VaidyanathanNoch keine Bewertungen
- Peer Graded AssignmentDokument3 SeitenPeer Graded Assignmentpadma100% (1)
- Teaching Acceptance Strategies Through Visualization PDFDokument2 SeitenTeaching Acceptance Strategies Through Visualization PDFVaibhav NahataNoch keine Bewertungen
- Competence of Mathematics Teachers in The Private Secondary Schools in The City of San Fernando, La Union: Basis For A Two-Pronged Training ProgramDokument245 SeitenCompetence of Mathematics Teachers in The Private Secondary Schools in The City of San Fernando, La Union: Basis For A Two-Pronged Training ProgramFeljone Ragma67% (3)
- Teaching Introductory Physics Arnold B AronsDokument5 SeitenTeaching Introductory Physics Arnold B AronsGanesh KumarNoch keine Bewertungen
- On Etulo IdeophonesDokument4 SeitenOn Etulo IdeophonesIOSRjournalNoch keine Bewertungen
- Conflict Resolution Lesson Plan 03Dokument4 SeitenConflict Resolution Lesson Plan 03api-396219108Noch keine Bewertungen
- Hermeneutic Philosophy of Science, Van Gogh'S Eyes, and GodDokument496 SeitenHermeneutic Philosophy of Science, Van Gogh'S Eyes, and Godagustinvolco9827100% (3)
- Daily Lesson Plan Overview Week 4 Friendly LetterDokument2 SeitenDaily Lesson Plan Overview Week 4 Friendly Letterapi-29831576Noch keine Bewertungen
- P.E. at Health PresentationDokument46 SeitenP.E. at Health PresentationMylene Quilatan Masanga100% (1)
- Messina ResumeDokument3 SeitenMessina Resumeapi-309413195Noch keine Bewertungen
- E10 Pang 1 Q3 - M1 QA PassedDokument17 SeitenE10 Pang 1 Q3 - M1 QA PassedBlessa Marel CaasiNoch keine Bewertungen
- Assig of English For Young Children.Dokument19 SeitenAssig of English For Young Children.S.ANNE MARY100% (1)
- Activity 4 - Knowing The TruthDokument10 SeitenActivity 4 - Knowing The TruthHenry BuemioNoch keine Bewertungen
- School Improvement Plans, A Tool To Improve The Quality of EducationDokument12 SeitenSchool Improvement Plans, A Tool To Improve The Quality of EducationArumugam ManickamNoch keine Bewertungen
- Model Konseptual Praktik Dalam Keperawatan Jiwa: Yulia Wardani, MANDokument21 SeitenModel Konseptual Praktik Dalam Keperawatan Jiwa: Yulia Wardani, MANDionisius KevinNoch keine Bewertungen
- Grid Literature ReviewDokument18 SeitenGrid Literature ReviewRexon GastonNoch keine Bewertungen
- JEC Curriculum Guide (BirthToThree)Dokument213 SeitenJEC Curriculum Guide (BirthToThree)Renice McFarlane74% (50)
- Lesson 5 Working Memory Model Ao3Dokument20 SeitenLesson 5 Working Memory Model Ao3Srnt YyoNoch keine Bewertungen
- Island in A Sea of SolitudeDokument4 SeitenIsland in A Sea of SolitudeRuth BergerNoch keine Bewertungen
- The Missing Peace in Your LifeDokument7 SeitenThe Missing Peace in Your Lifevia22Noch keine Bewertungen
- Iwai PDFDokument6 SeitenIwai PDFFSE HN - Giảng viên Tiếng Anh Đặng Thị Thanh VânNoch keine Bewertungen
- ReflectionDokument5 SeitenReflectionAmirahNoch keine Bewertungen
- How We Express Ourselves - Play 2016-17.PDF UpdatedDokument11 SeitenHow We Express Ourselves - Play 2016-17.PDF UpdatedSneha Mishra100% (1)
- Teaching Reading ScoreDokument3 SeitenTeaching Reading Scoreapi-403448804Noch keine Bewertungen
- 3 Traits and Characteristics of An EntreppreneurDokument31 Seiten3 Traits and Characteristics of An EntreppreneurAngelica LopezNoch keine Bewertungen
- Kapsch Resume January 2016Dokument1 SeiteKapsch Resume January 2016api-251092359Noch keine Bewertungen
- Leadership SummaryDokument3 SeitenLeadership SummaryBhagya ShreeNoch keine Bewertungen
- Social Process/ Learning Theories of CrimeDokument22 SeitenSocial Process/ Learning Theories of Crimebalal_hossain_1Noch keine Bewertungen