Das könnte Ihnen auch gefallen
- Nursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripDokument262 SeitenNursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripBheru LalNoch keine Bewertungen
- 2019 AM Functional Nutrition Assessment Presentation StrangeDokument61 Seiten2019 AM Functional Nutrition Assessment Presentation StrangeYasminNoch keine Bewertungen
- Health & IllnessDokument9 SeitenHealth & Illnesskayanmohamd506Noch keine Bewertungen
- Foods For Your Thoughts On Nutrition and Functional FoodsDokument40 SeitenFoods For Your Thoughts On Nutrition and Functional FoodsĐặng Nhật100% (1)
- Concept of Health and DiseaseDokument39 SeitenConcept of Health and DiseaseDr Izza AyubNoch keine Bewertungen
- Nutritional Assessment Methods in Clinical PracticeDokument28 SeitenNutritional Assessment Methods in Clinical PracticeESUFIYAN ALWSABINoch keine Bewertungen
- Nutritional AssessmentDokument18 SeitenNutritional AssessmentAliza ThakurNoch keine Bewertungen
- 1-Nutrition in NursingDokument31 Seiten1-Nutrition in NursingNedal AlhonityNoch keine Bewertungen
- 11 NDAprelimDokument6 Seiten11 NDAprelim2pwtqbcynjNoch keine Bewertungen
- Chapter 6 Nutrition Care ProcessDokument17 SeitenChapter 6 Nutrition Care Processr55fsf75hpNoch keine Bewertungen
- Weight Management: Common Tropical Infection - Tropical Medicine SystemDokument19 SeitenWeight Management: Common Tropical Infection - Tropical Medicine SystemMeilia N Chrisandra100% (1)
- 170910Dokument14 Seiten170910Mohona Rahman KhanNoch keine Bewertungen
- Health and Wellness ConceptsDokument38 SeitenHealth and Wellness ConceptsKathrina AlfonsoNoch keine Bewertungen
- Unit 1.1Dokument40 SeitenUnit 1.1Sunil RupjeeNoch keine Bewertungen
- Concept of Health and IllnessDokument28 SeitenConcept of Health and IllnessCeline Eliz Ang86% (7)
- Module 1: Health AssessmentDokument16 SeitenModule 1: Health AssessmentAmberNoch keine Bewertungen
- Topic 1 - Introduction To Nutrition in The Life Stages 1Dokument7 SeitenTopic 1 - Introduction To Nutrition in The Life Stages 1Aliyashir IbrahimNoch keine Bewertungen
- National University of Chimborazo Faculty of Health Sciences Clinical Psychology CareerDokument15 SeitenNational University of Chimborazo Faculty of Health Sciences Clinical Psychology CareerGisell AlmacheNoch keine Bewertungen
- Module 3 - Assessment of The Health StatusDokument43 SeitenModule 3 - Assessment of The Health StatusAYTONA, JAMAICA F.Noch keine Bewertungen
- Diabetes Mellitus Type 2Dokument20 SeitenDiabetes Mellitus Type 2Kylie GolindangNoch keine Bewertungen
- Group 2 Report in NutritionDokument99 SeitenGroup 2 Report in Nutritionfe espinosaNoch keine Bewertungen
- (Riazuddin)Dokument14 Seiten(Riazuddin)Mohona Rahman KhanNoch keine Bewertungen
- Chap 1 Health and WellnessDokument31 SeitenChap 1 Health and Wellnessapi-263590842Noch keine Bewertungen
- Chapter 15Dokument4 SeitenChapter 15Ed PascasioNoch keine Bewertungen
- Lesson 1 Beginning The AssessmentDokument36 SeitenLesson 1 Beginning The AssessmentAlex WindsorNoch keine Bewertungen
- Assessment of Nutritional Status - IDokument12 SeitenAssessment of Nutritional Status - ITamilarasan Arasur100% (1)
- Nutritional AssessmentDokument5 SeitenNutritional AssessmentimnasNoch keine Bewertungen
- How To Nutritional Assessment Revised PDFDokument9 SeitenHow To Nutritional Assessment Revised PDFHelina PedakNoch keine Bewertungen
- PlateletDokument16 SeitenPlateletArgene Rose MilletNoch keine Bewertungen
- MODELS (1)Dokument14 SeitenMODELS (1)sswweettii23Noch keine Bewertungen
- Part 1Dokument8 SeitenPart 1api-437831510Noch keine Bewertungen
- Nutrition Intervention 1111Dokument34 SeitenNutrition Intervention 1111Angel Grace Miranda100% (1)
- Nursing Health HistoryDokument11 SeitenNursing Health Historyrubycorazon_edizaNoch keine Bewertungen
- module-3-PE-Health 3rdyearDokument15 Seitenmodule-3-PE-Health 3rdyearAngelica SaczNoch keine Bewertungen
- Food Habits And Awareness Among Adolescent StudentsDokument6 SeitenFood Habits And Awareness Among Adolescent StudentsAparnaaVenkatesanNoch keine Bewertungen
- Health and Wellness FINALDokument54 SeitenHealth and Wellness FINALsarah alzg100% (1)
- Introduction Ho-1Dokument282 SeitenIntroduction Ho-1TEWODROS TADDESENoch keine Bewertungen
- Health BeliefDokument30 SeitenHealth BeliefHemantNoch keine Bewertungen
- LWW - Bates - 05 - General Survey - Transcript - FinalDokument8 SeitenLWW - Bates - 05 - General Survey - Transcript - FinalMary AmaliaNoch keine Bewertungen
- CHN I Overview of Public Health in the PhilippinesDokument13 SeitenCHN I Overview of Public Health in the Philippinesjohncarlo ramosNoch keine Bewertungen
- Understanding Patients and Health ConceptsDokument8 SeitenUnderstanding Patients and Health ConceptsMaan EspirituNoch keine Bewertungen
- Nutritional Needs of A Client: by Mr. Manasseh Mvula 4 Year BSC StudentDokument31 SeitenNutritional Needs of A Client: by Mr. Manasseh Mvula 4 Year BSC StudentJonnalagadda MiryaniNoch keine Bewertungen
- Cues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationDokument6 SeitenCues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationKatrina Ponce86% (7)
- To Understand The Consumer Behaviour With RespectDokument13 SeitenTo Understand The Consumer Behaviour With RespectSandal Deep SaraoNoch keine Bewertungen
- Health and IllnessDokument6 SeitenHealth and Illnessmichaella pizarroNoch keine Bewertungen
- 2nutritionassmt Studay1819Dokument101 Seiten2nutritionassmt Studay1819RaysonChoo100% (2)
- Concepts of Health Wellness and Well BeingDokument6 SeitenConcepts of Health Wellness and Well Beinglai.creates4uNoch keine Bewertungen
- Module 3 Food & NutritionDokument15 SeitenModule 3 Food & NutritionPJ ProcoratoNoch keine Bewertungen
- Cl.8 U.4L.3 Never Give UpDokument6 SeitenCl.8 U.4L.3 Never Give UpAlina CebotariNoch keine Bewertungen
- Man, Health, & Illness: InsertDokument50 SeitenMan, Health, & Illness: InsertJan Oliver YaresNoch keine Bewertungen
- Assess Nutritional Status MethodsDokument46 SeitenAssess Nutritional Status MethodsSalmaNoch keine Bewertungen
- Teori Florence NightingaleDokument16 SeitenTeori Florence NightingaleUcokNoch keine Bewertungen
- Health Wellness and IllnessDokument42 SeitenHealth Wellness and IllnessTwesigye DeusNoch keine Bewertungen
- Nutrition Nursing: Food, Nutrition HealthDokument27 SeitenNutrition Nursing: Food, Nutrition HealthAngelyka Nicole Bengco David100% (1)
- Nutrition AssessmentDokument47 SeitenNutrition AssessmentMohamed F. Nada100% (6)
- CaseDokument16 SeitenCaseJesil MarolinaNoch keine Bewertungen
- The Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingVon EverandThe Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingNoch keine Bewertungen
- Mindful Nourishment: Holistic Approach To Eating Disorders.Von EverandMindful Nourishment: Holistic Approach To Eating Disorders.Noch keine Bewertungen
- Nourish A Comprehensive Guide to Healthy Eating and Sustainable LivingVon EverandNourish A Comprehensive Guide to Healthy Eating and Sustainable LivingNoch keine Bewertungen
- Lecture 3 Medical Parasitology and MicrobiolgyDokument6 SeitenLecture 3 Medical Parasitology and Microbiolgyabdirahman NoahNoch keine Bewertungen
- Lecture 2 Medical Parasitology and MicrobiolgyDokument11 SeitenLecture 2 Medical Parasitology and Microbiolgyabdirahman NoahNoch keine Bewertungen
- Lecture 1 Medical Parasitology and MicrobiolgyDokument7 SeitenLecture 1 Medical Parasitology and Microbiolgyabdirahman NoahNoch keine Bewertungen
- Parasitology Chapter 6Dokument73 SeitenParasitology Chapter 6abdirahman NoahNoch keine Bewertungen
- Presentation Group One BoysDokument32 SeitenPresentation Group One Boysabdirahman NoahNoch keine Bewertungen
- Overactive Bladder - Concept-Map - Jesoro - JM - P. - 2BSN2Dokument2 SeitenOveractive Bladder - Concept-Map - Jesoro - JM - P. - 2BSN2Jane Mae JesoroNoch keine Bewertungen
- Analysing Seasonal Health DataDokument174 SeitenAnalysing Seasonal Health DataIsmailNoch keine Bewertungen
- Ladder Risk AssessmentDokument3 SeitenLadder Risk AssessmentPearl TeresaNoch keine Bewertungen
- Covid-19, A Black Swan Event Managing Supply Chain Risk and DisruptionDokument2 SeitenCovid-19, A Black Swan Event Managing Supply Chain Risk and DisruptionUmer RehmanNoch keine Bewertungen
- Abdominal Trauma PDFDokument17 SeitenAbdominal Trauma PDFCarlos UrquijoNoch keine Bewertungen
- Surgery Practical What To ExpectDokument4 SeitenSurgery Practical What To ExpectNirbhay100% (1)
- Fit Report RedactedDokument28 SeitenFit Report RedactedLas Vegas Review-JournalNoch keine Bewertungen
- Lesson Plan 2021-2022 FinalDokument6 SeitenLesson Plan 2021-2022 FinalJANETH ASISNoch keine Bewertungen
- Basics of Electrotherapy 2ndDokument175 SeitenBasics of Electrotherapy 2ndSilvano Cardona92% (13)
- Cholera A Worldwide HistoryDokument407 SeitenCholera A Worldwide HistoryRiccardo MazzelliNoch keine Bewertungen
- Chain of InfectionDokument3 SeitenChain of InfectionShaina SantosNoch keine Bewertungen
- Clinical Review: Emergency Medicine Myths: Cerebral Edema in Pediatric Diabetic Ketoacidosis and Intravenous FluidsDokument10 SeitenClinical Review: Emergency Medicine Myths: Cerebral Edema in Pediatric Diabetic Ketoacidosis and Intravenous FluidsKaye NeeNoch keine Bewertungen
- Essay-Mike Lemuel BacayoDokument1 SeiteEssay-Mike Lemuel BacayoLem MikeeNoch keine Bewertungen
- Prevent Strokes: Learn Signs, Risks and Lifestyle ChangesDokument10 SeitenPrevent Strokes: Learn Signs, Risks and Lifestyle Changesjericho dinglasanNoch keine Bewertungen
- 2019, Volume 6, No 1: ISSN 2397-5628Dokument46 Seiten2019, Volume 6, No 1: ISSN 2397-5628djonoumaNoch keine Bewertungen
- Acute Appendicitis: Surgical PostingDokument8 SeitenAcute Appendicitis: Surgical PostingGraldoNoch keine Bewertungen
- Contaminated Drinking Water As A Risk Factor For Colibacilosis - PlusVet Animal HealthDokument8 SeitenContaminated Drinking Water As A Risk Factor For Colibacilosis - PlusVet Animal HealthEduardo ViolaNoch keine Bewertungen
- E.coli SmitaDokument40 SeitenE.coli SmitaNeha SinhaNoch keine Bewertungen
- Bescos (2020), Effects of Chlorhexidine Mouthwash On The Oral MicrobiomeDokument8 SeitenBescos (2020), Effects of Chlorhexidine Mouthwash On The Oral MicrobiomePhuong ThaoNoch keine Bewertungen
- WCPSS Student Health GuidanceDokument7 SeitenWCPSS Student Health GuidanceKeung HuiNoch keine Bewertungen
- F.SARAWI NCP SIC Drug StudyDokument30 SeitenF.SARAWI NCP SIC Drug StudyaldwinNoch keine Bewertungen
- Apple of Sodom Facts and Health BenefitsDokument2 SeitenApple of Sodom Facts and Health BenefitsUmarion FarukanNoch keine Bewertungen
- Urine Culture Manual MT - SINAI PDFDokument15 SeitenUrine Culture Manual MT - SINAI PDFAvi VermaNoch keine Bewertungen
- 1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-ConceptionDokument2 Seiten1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-Conceptionjoel TorresNoch keine Bewertungen
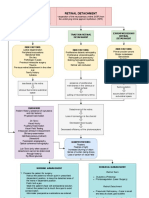
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDokument3 SeitenRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- 4CLCZrVWEemNrQqD1GEKdA - Botanicals For Womens Health Reference Sheet - v2Dokument2 Seiten4CLCZrVWEemNrQqD1GEKdA - Botanicals For Womens Health Reference Sheet - v2Ximena CastexNoch keine Bewertungen
- A Study On The Correlation of ABO Blood Group System and HypertensionDokument4 SeitenA Study On The Correlation of ABO Blood Group System and HypertensionHema SinghNoch keine Bewertungen
- Anemia - AMBOSSDokument2 SeitenAnemia - AMBOSStgayuNoch keine Bewertungen
- Plasma ProteinsDokument8 SeitenPlasma ProteinsAaryan50% (2)
- Path To Improved Health: Physical Health - Taking Care of Your BodyDokument6 SeitenPath To Improved Health: Physical Health - Taking Care of Your BodyMaria Katrinka Sophia MartiresNoch keine Bewertungen