Das könnte Ihnen auch gefallen
- Medical Terminology For Health Professions 7th Edition Ehrlich Solutions Manual 1Dokument24 SeitenMedical Terminology For Health Professions 7th Edition Ehrlich Solutions Manual 1leroy100% (50)
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)Von EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)Noch keine Bewertungen
- Ischemic Heart DiseaseDokument67 SeitenIschemic Heart Diseasealfaz lakhani80% (5)
- Anatomy Myocardial InfarctionDokument5 SeitenAnatomy Myocardial InfarctionLyka Milo AvilaNoch keine Bewertungen
- Types of Cardiovascular Disease in The HeartDokument7 SeitenTypes of Cardiovascular Disease in The Heartissey1652Noch keine Bewertungen
- 10 - FN 14 CVS Anatomy IntroDokument15 Seiten10 - FN 14 CVS Anatomy IntroCamille GrefaldiaNoch keine Bewertungen
- Spanish Medical GlossaryDokument129 SeitenSpanish Medical GlossaryAlex ObandoNoch keine Bewertungen
- Cardiogenic Shock: Historical AspectsDokument24 SeitenCardiogenic Shock: Historical AspectsnugessurNoch keine Bewertungen
- Heart Failure: A Case AnalysisDokument14 SeitenHeart Failure: A Case AnalysisBrix ValdrizNoch keine Bewertungen
- The HeartDokument36 SeitenThe HeartMuskan Bisht100% (3)
- Congestive Heart Failure. Case Study ExplanationDokument6 SeitenCongestive Heart Failure. Case Study ExplanationOkenabirhie100% (1)
- Basic Tablet Coating Technology-2013-3yr-3e-Part-B PDFDokument52 SeitenBasic Tablet Coating Technology-2013-3yr-3e-Part-B PDFAli Akand AsifNoch keine Bewertungen
- Lecture 2 Ischemic Heart DiseasesDokument19 SeitenLecture 2 Ischemic Heart DiseasesOsama MalikNoch keine Bewertungen
- CardiomyopathyDokument98 SeitenCardiomyopathyZellanien hdNoch keine Bewertungen
- Myocardial Ischemia: Dr. Wael H. Mansy, MDDokument37 SeitenMyocardial Ischemia: Dr. Wael H. Mansy, MDHaleema SultanNoch keine Bewertungen
- Heart FailureDokument13 SeitenHeart Failuremildred alidon100% (2)
- Hypertensive Heart DiseaseDokument18 SeitenHypertensive Heart DiseaseAmanda Edwards100% (1)
- In Partial Fulfillment of The Requirements in Medical Ward RotationDokument5 SeitenIn Partial Fulfillment of The Requirements in Medical Ward RotationEiz CabreraNoch keine Bewertungen
- Cardio Myopathy.Dokument17 SeitenCardio Myopathy.Salman Khan100% (1)
- Ischemic Heart DiseaseDokument5 SeitenIschemic Heart DiseaseBert DivinagraciaNoch keine Bewertungen
- PRINTED Cardiovascular System (Heart) HandoutsDokument7 SeitenPRINTED Cardiovascular System (Heart) HandoutsKate GutierrezNoch keine Bewertungen
- Color Atlas of PathologyDokument485 SeitenColor Atlas of PathologyMarcelo Coelho100% (1)
- Cultivation of BacteriaDokument27 SeitenCultivation of BacteriaAli Akand Asif50% (2)
- An Introduction To Autopsy Technique: Step-by-Step DiagramsDokument24 SeitenAn Introduction To Autopsy Technique: Step-by-Step Diagramskarin45Noch keine Bewertungen
- Coronary Artery DiseaseDokument3 SeitenCoronary Artery DiseaseAlan Valencia Baya Jr.Noch keine Bewertungen
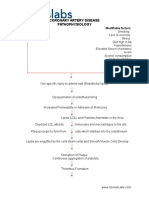
- Coronary Artery Disease PathophysiologyDokument3 SeitenCoronary Artery Disease Pathophysiologynursing concept maps50% (4)
- Case Study EssayDokument19 SeitenCase Study EssaylecharmedenuitNoch keine Bewertungen
- NP3 4Dokument65 SeitenNP3 4Edward Nicko Garcia100% (1)
- Basic Coronary Angiography - All Slides PDFDokument55 SeitenBasic Coronary Angiography - All Slides PDFCarlos Arroyo0% (1)
- Cardiovascular Diseases Management Amp Nursing CareDokument76 SeitenCardiovascular Diseases Management Amp Nursing CareAlberto MeroNoch keine Bewertungen
- CardioDokument6 SeitenCardioGrace GurdielNoch keine Bewertungen
- IntroductionDokument13 SeitenIntroductionSiyara AntonyNoch keine Bewertungen
- Heart FailureDokument39 SeitenHeart FailureMuhammad AsifNoch keine Bewertungen
- Introduction - MIDokument10 SeitenIntroduction - MIkhimiiiNoch keine Bewertungen
- Heart Guide 2022Dokument13 SeitenHeart Guide 2022AnuNoch keine Bewertungen
- 3 IschemicHeartDiseasesDokument17 Seiten3 IschemicHeartDiseasesHarsha MaheshwariNoch keine Bewertungen
- (311 - Rakshita) (312 - Aashish Bharti) - There Are Six Principal Mechanisms of Cardiovascular DysfunctionDokument15 Seiten(311 - Rakshita) (312 - Aashish Bharti) - There Are Six Principal Mechanisms of Cardiovascular DysfunctionAyshwarya LalNoch keine Bewertungen
- Biologic Crisis:: Prepared By: Recitas, Anna Lou G. BSN-4 Sn-DoscstDokument64 SeitenBiologic Crisis:: Prepared By: Recitas, Anna Lou G. BSN-4 Sn-DoscstDonna Solamo TalabocNoch keine Bewertungen
- Neacsu Aurelia EssayDokument3 SeitenNeacsu Aurelia EssaySimona NeacsuNoch keine Bewertungen
- Ischemic Cardiac Conditions Cardiac Muscle Dysfunction: Dr. Afaq Ahmad PT Cardiopulmonary Physical TherapyDokument19 SeitenIschemic Cardiac Conditions Cardiac Muscle Dysfunction: Dr. Afaq Ahmad PT Cardiopulmonary Physical TherapyHUSNAIN TECH AND FUNNoch keine Bewertungen
- Angina Pectoris Myocardial Infarction: Bahuguna, Nimisha Imd-Batch 3Dokument19 SeitenAngina Pectoris Myocardial Infarction: Bahuguna, Nimisha Imd-Batch 3Nimisha BahugunaNoch keine Bewertungen
- Heart FailureDokument61 SeitenHeart Failurehadushnl770Noch keine Bewertungen
- Patho 1Dokument153 SeitenPatho 1ademabdellaaleNoch keine Bewertungen
- General Diseases and Conditions Aortic DissectionDokument5 SeitenGeneral Diseases and Conditions Aortic DissectionCambo BishtosNoch keine Bewertungen
- Angelina A Joho MSC in Critical Care and TraumaDokument50 SeitenAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNoch keine Bewertungen
- Atherosclerosis and Myocardial InfractionDokument26 SeitenAtherosclerosis and Myocardial InfractionElina GNoch keine Bewertungen
- 4 - (CHF), IschemicDokument31 Seiten4 - (CHF), IschemicLobna ElkilanyNoch keine Bewertungen
- HemopericardiumDokument1 SeiteHemopericardiumlourdesfercab_at_msnNoch keine Bewertungen
- Cardiology 3 F2018Dokument34 SeitenCardiology 3 F2018TkNoch keine Bewertungen
- HHFFDokument56 SeitenHHFFNesru Ahmed AkkichuNoch keine Bewertungen
- Cardiovascular DisorderDokument4 SeitenCardiovascular Disorderhxqf25mbvvNoch keine Bewertungen
- Case 2 SlosDokument7 SeitenCase 2 SlosNamarNoch keine Bewertungen
- 18 Heartpart1 Basiccongestiveheartfailure 110919083613 Phpapp01Dokument43 Seiten18 Heartpart1 Basiccongestiveheartfailure 110919083613 Phpapp01Atikah PurnamasariNoch keine Bewertungen
- Cardio MyopathiesDokument39 SeitenCardio Myopathiesinyanji.barasaNoch keine Bewertungen
- CardiomyopathyDokument17 SeitenCardiomyopathyRashed ShatnawiNoch keine Bewertungen
- نسخة HeartDokument29 Seitenنسخة HeartKyunaNoch keine Bewertungen
- Valvular Heart Disease: Dr. Nigussie BerihunDokument43 SeitenValvular Heart Disease: Dr. Nigussie Berihunsisay tigabuNoch keine Bewertungen
- Cardiovascular Disease: Coronary Heart Disease Refers To The Failure of The Coronary Circulation To Supply AdequateDokument4 SeitenCardiovascular Disease: Coronary Heart Disease Refers To The Failure of The Coronary Circulation To Supply AdequateAnant Kumar SrivastavaNoch keine Bewertungen
- Lecture 1 Heart OverviewDokument20 SeitenLecture 1 Heart OverviewOsama MalikNoch keine Bewertungen
- 19 Cardiac DisordersDokument51 Seiten19 Cardiac DisordersChessie Garcia100% (1)
- Heart FailureDokument61 SeitenHeart FailureGideon HaburaNoch keine Bewertungen
- LO Dan WO Cardio Week 4 (Jumat)Dokument38 SeitenLO Dan WO Cardio Week 4 (Jumat)Alan Dwi SetiawanNoch keine Bewertungen
- EscardioDokument9 SeitenEscardioMYMANoch keine Bewertungen
- Cardiogenic ShockDokument26 SeitenCardiogenic ShockAnggun V. M SitumorangNoch keine Bewertungen
- 20cardiac Broken HeartDokument16 Seiten20cardiac Broken HeartJaydave PatelNoch keine Bewertungen
- Anti Ischemic DrugsDokument33 SeitenAnti Ischemic Drugsdeepak askarNoch keine Bewertungen
- The Heart-1Dokument30 SeitenThe Heart-1Ebuka AniNoch keine Bewertungen
- Myocardial Infarction: BackgroundDokument9 SeitenMyocardial Infarction: BackgroundNor Faizah Ahmad SadriNoch keine Bewertungen
- Disorders of The Circulatory SystemDokument3 SeitenDisorders of The Circulatory SystemCondurache Ilie-AndreiNoch keine Bewertungen
- PR 3Dokument14 SeitenPR 3Sri PurwantiNoch keine Bewertungen
- %VVVVVV VV %VVVVVV %VVV VVV VDokument8 Seiten%VVVVVV VV %VVVVVV %VVV VVV VKris Joy AdriculaNoch keine Bewertungen
- Coronary Artery DisaeseDokument48 SeitenCoronary Artery DisaeseAzkaZulfiqarNoch keine Bewertungen
- Gagal JantungDokument69 SeitenGagal JantungKota Tako100% (1)
- Cardiomyopathies: Cardiomyopathy Is A Heart Muscle Disease Associated With CardiacDokument10 SeitenCardiomyopathies: Cardiomyopathy Is A Heart Muscle Disease Associated With Cardiacmerin sunilNoch keine Bewertungen
- Hypophysis CerebriDokument21 SeitenHypophysis CerebriAli Akand AsifNoch keine Bewertungen
- Physical Agents Chemical AgentsDokument47 SeitenPhysical Agents Chemical AgentsAli Akand AsifNoch keine Bewertungen
- EWU Evolution of PharmacyDokument16 SeitenEWU Evolution of PharmacyAli Akand Asif100% (1)
- History of PharmacyDokument42 SeitenHistory of PharmacyAli Akand AsifNoch keine Bewertungen
- Medicinal Gases 03Dokument9 SeitenMedicinal Gases 03Ali Akand Asif0% (1)
- Chapter One: Historical Development of ComputersDokument20 SeitenChapter One: Historical Development of ComputersAli Akand AsifNoch keine Bewertungen
- Carboxylic Acids (MRH)Dokument49 SeitenCarboxylic Acids (MRH)Ali Akand AsifNoch keine Bewertungen
- Name Eactions FinalDokument33 SeitenName Eactions FinalAli Akand AsifNoch keine Bewertungen
- SM Chapter 2Dokument34 SeitenSM Chapter 2Ali Akand AsifNoch keine Bewertungen
- Overview On TranscriptionDokument21 SeitenOverview On TranscriptionAli Akand AsifNoch keine Bewertungen
- Thesis Paper Writing (Result and Discussion)Dokument43 SeitenThesis Paper Writing (Result and Discussion)Ali Akand AsifNoch keine Bewertungen
- RNA Extraction Is The Purification ofDokument3 SeitenRNA Extraction Is The Purification ofAli Akand Asif100% (1)
- DNA Extraction: DNA Isolation Is A Routine Procedure To CollectDokument3 SeitenDNA Extraction: DNA Isolation Is A Routine Procedure To CollectAli Akand AsifNoch keine Bewertungen
- Distribution of DrugsDokument20 SeitenDistribution of DrugsAli Akand AsifNoch keine Bewertungen
- SM Chapter 1Dokument17 SeitenSM Chapter 1Ali Akand AsifNoch keine Bewertungen
- Plant Layout of PharmaceuticalsDokument20 SeitenPlant Layout of PharmaceuticalsAli Akand AsifNoch keine Bewertungen
- Business Model of Evaly: Evaly's Strategies For Generate Revenue (Source of Income)Dokument3 SeitenBusiness Model of Evaly: Evaly's Strategies For Generate Revenue (Source of Income)Ali Akand AsifNoch keine Bewertungen
- Aminoglycosides: Amlan GangulyDokument14 SeitenAminoglycosides: Amlan GangulyAli Akand AsifNoch keine Bewertungen
- M6 PDFDokument43 SeitenM6 PDFAli Akand AsifNoch keine Bewertungen
- It Infrastructure and Emerging Technologies: Dr. Mohammad Naveed AhmedDokument47 SeitenIt Infrastructure and Emerging Technologies: Dr. Mohammad Naveed AhmedAli Akand AsifNoch keine Bewertungen
- 2015 - Stereochemistry-II (MRH) DUDokument73 Seiten2015 - Stereochemistry-II (MRH) DUAli Akand AsifNoch keine Bewertungen
- Mixing: Md. Shahadat Hossain Dept. of Pharmaceutical TechnologyDokument25 SeitenMixing: Md. Shahadat Hossain Dept. of Pharmaceutical TechnologyAli Akand AsifNoch keine Bewertungen
- NEET PG 2012 Question Paper With SolutionsDokument1.588 SeitenNEET PG 2012 Question Paper With Solutionssejal3vijNoch keine Bewertungen
- CABG PCS CodingDokument3 SeitenCABG PCS CodingVikas MaheshwariNoch keine Bewertungen
- Pediatric Cardiopulmonary ResuscitationDokument15 SeitenPediatric Cardiopulmonary ResuscitationGhiza Ainurrahmah BawafieNoch keine Bewertungen
- Humoral and Intra Cardiac Mechanism of Heart' RegulationDokument23 SeitenHumoral and Intra Cardiac Mechanism of Heart' RegulationAman singhNoch keine Bewertungen
- Project BioDokument18 SeitenProject Bioyanshu falduNoch keine Bewertungen
- Cardiovascular System Anatomy and Physiology - Study Guide For NursesDokument34 SeitenCardiovascular System Anatomy and Physiology - Study Guide For NursesMarie ParksNoch keine Bewertungen
- Acute Coronary Syndrome Case-Report: A U F Angeles City College of NursingDokument77 SeitenAcute Coronary Syndrome Case-Report: A U F Angeles City College of NursingCarlo Joseph Intal LlacerNoch keine Bewertungen
- Human Physiology 14th Edition Fox Solutions ManualDokument16 SeitenHuman Physiology 14th Edition Fox Solutions Manualoraliemaximusp474w3100% (28)
- Ati Teas 7 Anatomy and Physiology Review With Questions and AnswersDokument48 SeitenAti Teas 7 Anatomy and Physiology Review With Questions and AnswersSAMUEL WAMNoch keine Bewertungen
- Chap 26 To 38 Case Study Answers To QuestionsDokument13 SeitenChap 26 To 38 Case Study Answers To QuestionsElaine Jean UayanNoch keine Bewertungen
- Circulatory SystemDokument21 SeitenCirculatory SystemSaadNoch keine Bewertungen
- Pathmorpho2nd 1Dokument1 SeitePathmorpho2nd 1Hart ElettNoch keine Bewertungen
- Test Bank For Basic Medical Language 4th Edition Lafleur DownloadDokument13 SeitenTest Bank For Basic Medical Language 4th Edition Lafleur Downloadantoniowagnercrqampebwt100% (29)
- PathologyDokument28 SeitenPathologyakkashamrishNoch keine Bewertungen
- Etextbook PDF For Study Guide For Pathophysiology The Biological Basis For Disease in Adults and Children 8th EditionDokument62 SeitenEtextbook PDF For Study Guide For Pathophysiology The Biological Basis For Disease in Adults and Children 8th Editionreynaldo.bailey262100% (39)
- Case Study 2 - FinishedDokument12 SeitenCase Study 2 - Finishedapi-307945760Noch keine Bewertungen
- Cardiac Rehab BookletDokument14 SeitenCardiac Rehab BookletansarijavedNoch keine Bewertungen
- Anaphy LectureDokument68 SeitenAnaphy LectureZoe AlexanderNoch keine Bewertungen