Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- DR - BD S Step 1 Guide - PDF Filename UTF-8 DR - BD S Step 1 GuideDokument24 SeitenDR - BD S Step 1 Guide - PDF Filename UTF-8 DR - BD S Step 1 GuideAdeelMunawarNoch keine Bewertungen
- Overview of Nervous SystemDokument63 SeitenOverview of Nervous SystemMAHARANI100% (1)
- How to Dilute Blood and Count White Blood CellsDokument2 SeitenHow to Dilute Blood and Count White Blood CellsAlfred ChowNoch keine Bewertungen
- Levels of Organization Power Point and ActivityDokument8 SeitenLevels of Organization Power Point and ActivityJudy RianoNoch keine Bewertungen
- The Breath of Yoga & Martial ArtsDokument15 SeitenThe Breath of Yoga & Martial Artskarynchin100% (2)
- 3 Piece Intrusion Arch - Bhavana ShroffDokument8 Seiten3 Piece Intrusion Arch - Bhavana ShroffSai Seshadri Bharath ThotaNoch keine Bewertungen
- How Your Diet Affects Your BrainDokument2 SeitenHow Your Diet Affects Your BrainRusso Dalmasso50% (2)
- Infectiile de tract urinar: cazuri cliniceDokument55 SeitenInfectiile de tract urinar: cazuri cliniceMădălina Mihaela LuchianNoch keine Bewertungen
- Importance of Anaerobic Glycolysis & Stiffness in SprintsDokument7 SeitenImportance of Anaerobic Glycolysis & Stiffness in SprintsAltec AlsingNoch keine Bewertungen
- Stoichiometry of Microbial Growth and Product FormationDokument10 SeitenStoichiometry of Microbial Growth and Product FormationfayeNoch keine Bewertungen
- Endocrine Emergencies CompiledDokument102 SeitenEndocrine Emergencies CompiledSubhkanish RavindraNoch keine Bewertungen
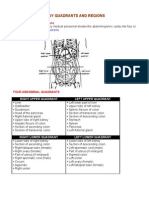
- Organs in The Body Quadrants and RegionsDokument3 SeitenOrgans in The Body Quadrants and RegionsDavid HosamNoch keine Bewertungen
- 2992-Article Text-8831-1-10-20220715Dokument8 Seiten2992-Article Text-8831-1-10-20220715umbu anandaNoch keine Bewertungen
- COVID-19 Infection in Pregnant Women: Review of Maternal and Fetal OutcomesDokument8 SeitenCOVID-19 Infection in Pregnant Women: Review of Maternal and Fetal Outcomesumbu anandaNoch keine Bewertungen
- Covid 19 in Pregnancy: Risk of Adverse Neonatal Outcomes: LettertotheeditorDokument3 SeitenCovid 19 in Pregnancy: Risk of Adverse Neonatal Outcomes: Lettertotheeditorumbu anandaNoch keine Bewertungen
- Clinical Microbiology and InfectionDokument3 SeitenClinical Microbiology and Infectionumbu anandaNoch keine Bewertungen
- Coronavirus Disease 2019 (COVID-19) Pandemic and Pregnancy: Pradip - Dashraath - Vijayakumar@nuhs - Edu.sgDokument11 SeitenCoronavirus Disease 2019 (COVID-19) Pandemic and Pregnancy: Pradip - Dashraath - Vijayakumar@nuhs - Edu.sgMedecinBissMedNoch keine Bewertungen
- Placental Sars Cov 2 in A Pregnant Woman With Mild Covid 19 DiseaseDokument7 SeitenPlacental Sars Cov 2 in A Pregnant Woman With Mild Covid 19 Diseaseumbu anandaNoch keine Bewertungen
- Maternal Death in Pregnancy Due To COVID-19: CorrespondenceDokument1 SeiteMaternal Death in Pregnancy Due To COVID-19: Correspondenceumbu anandaNoch keine Bewertungen
- Webinar Forkom DR Peduli Covid-19Dokument40 SeitenWebinar Forkom DR Peduli Covid-19umbu anandaNoch keine Bewertungen
- AV Shunt PDFDokument16 SeitenAV Shunt PDFumbu anandaNoch keine Bewertungen
- Fungsi Otot-OtotDokument32 SeitenFungsi Otot-OtothansenpanjaitanNoch keine Bewertungen
- Proprioceptive Training HandballDokument23 SeitenProprioceptive Training HandballRoginicD100% (1)
- PBL Biochem Lab - EnzymesDokument4 SeitenPBL Biochem Lab - EnzymesGren May Angeli MagsakayNoch keine Bewertungen
- Revision Sheet Grade 5 For Ut1Dokument5 SeitenRevision Sheet Grade 5 For Ut1Sudeep BhattacharyaNoch keine Bewertungen
- Some Answer of Problemset - 7 - KEYDokument3 SeitenSome Answer of Problemset - 7 - KEYNihir PatelNoch keine Bewertungen
- Hematological and Metabolical Aspects From Laboratory MediDokument109 SeitenHematological and Metabolical Aspects From Laboratory MediNadirNoch keine Bewertungen
- Eng Hamid & Zakaria PDFDokument5 SeitenEng Hamid & Zakaria PDFTiga TujuhNoch keine Bewertungen
- Veta 3 - Datasheet - ENG - 20210315Dokument2 SeitenVeta 3 - Datasheet - ENG - 20210315JuanNoch keine Bewertungen
- Frog Dissection (Remote)Dokument21 SeitenFrog Dissection (Remote)Mohammad NiyaifarNoch keine Bewertungen
- J. Biol. Chem.-1953-Forbes-359-66Dokument9 SeitenJ. Biol. Chem.-1953-Forbes-359-66Fachrun SofiyahNoch keine Bewertungen
- ElectrocardiographyDokument21 SeitenElectrocardiographyTol Man ShresthaNoch keine Bewertungen
- Drug StudiesDokument32 SeitenDrug StudiesKelly ChanNoch keine Bewertungen
- Finney Ms Case StudyDokument17 SeitenFinney Ms Case Studyapi-255767391Noch keine Bewertungen
- TonsillectomyDokument27 SeitenTonsillectomyRho Vince Caño MalagueñoNoch keine Bewertungen
- Auditory Pathways: Anatomy and Physiology: Handbook of Clinical Neurology March 2015Dokument24 SeitenAuditory Pathways: Anatomy and Physiology: Handbook of Clinical Neurology March 2015florensiaNoch keine Bewertungen
- TRACHEA With TransDokument56 SeitenTRACHEA With TransLarry YuloNoch keine Bewertungen
- Identify The Part of The BrainDokument2 SeitenIdentify The Part of The BrainClement Mar ClimacoNoch keine Bewertungen
- Blood Cell MorphologyDokument5 SeitenBlood Cell MorphologyKIPRUTO DENNISNoch keine Bewertungen