Das könnte Ihnen auch gefallen
- Typology of Learners With Special Needs: " Know The Types and Know Your Rights "Dokument74 SeitenTypology of Learners With Special Needs: " Know The Types and Know Your Rights "Shai MacapillarNoch keine Bewertungen
- Typology of Learners With Special Needs: " Know The Types and Know Your Rights "Dokument67 SeitenTypology of Learners With Special Needs: " Know The Types and Know Your Rights "Shai MacapillarNoch keine Bewertungen
- Group 4Dokument67 SeitenGroup 4Shai MacapillarNoch keine Bewertungen
- Intellectual Disability (Down Syndrome)Dokument23 SeitenIntellectual Disability (Down Syndrome)Rodrigo RuizNoch keine Bewertungen
- Group 4: EED 33 1-Foun Dation of Speci Al & Inc Lusive Educati OnDokument20 SeitenGroup 4: EED 33 1-Foun Dation of Speci Al & Inc Lusive Educati OnShai MacapillarNoch keine Bewertungen
- Diagnose Van DyslexieDokument1 SeiteDiagnose Van DyslexiePeter Van GilsNoch keine Bewertungen
- Typology of Learners With Special Needs: " Know The Types and Know Your Rights "Dokument67 SeitenTypology of Learners With Special Needs: " Know The Types and Know Your Rights "Shai MacapillarNoch keine Bewertungen
- Dreams Are Something To Work For, Not Something To Wait For!Dokument46 SeitenDreams Are Something To Work For, Not Something To Wait For!Vijayakanth VijayakumarNoch keine Bewertungen
- Group 4: EED 33 1-Foundatio N of Spec Ial & Inclus Ive Educa TionDokument20 SeitenGroup 4: EED 33 1-Foundatio N of Spec Ial & Inclus Ive Educa TionShai MacapillarNoch keine Bewertungen
- Educ 148 Chapter III A To DDokument100 SeitenEduc 148 Chapter III A To DMichelle YadaoNoch keine Bewertungen
- Dementia - A Way Ahead: A user-friendly guide for dementia enriched with therapeutic information to assist & empower family & carersVon EverandDementia - A Way Ahead: A user-friendly guide for dementia enriched with therapeutic information to assist & empower family & carersNoch keine Bewertungen
- BBMS3011 Autism and SchizophreniaDokument32 SeitenBBMS3011 Autism and Schizophreniakeven319hk4304Noch keine Bewertungen
- Final Service Map Reach For The StarsDokument28 SeitenFinal Service Map Reach For The Starsapi-317697196Noch keine Bewertungen
- Seminar DementiaDokument63 SeitenSeminar DementiaAhmad Syahmi YZNoch keine Bewertungen
- What Is Alzheimer's Disease?: Amyloid Plaques, Which Are Made Up of Fragments of A Protein Called BetaDokument8 SeitenWhat Is Alzheimer's Disease?: Amyloid Plaques, Which Are Made Up of Fragments of A Protein Called BetavicmomNoch keine Bewertungen
- Child Psychiatry1Dokument21 SeitenChild Psychiatry1mariam tarekNoch keine Bewertungen
- Assessment Task3: Empowering Disabled People (CHCDIS007)Dokument6 SeitenAssessment Task3: Empowering Disabled People (CHCDIS007)Ashesh BasnetNoch keine Bewertungen
- Espejon. Project3.PROFED05 PDFDokument22 SeitenEspejon. Project3.PROFED05 PDFMichael John Paul EspejonNoch keine Bewertungen
- NCM 109 Reviewer Module 1Dokument6 SeitenNCM 109 Reviewer Module 1tamsmadjad18Noch keine Bewertungen
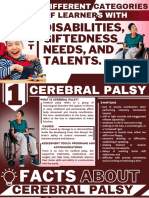
- Cerebral PalsyDokument21 SeitenCerebral Palsynwogu.kamsiyoNoch keine Bewertungen
- Physical Education and Sports For CWSN (Children With Special Needs - (Divyanag)Dokument19 SeitenPhysical Education and Sports For CWSN (Children With Special Needs - (Divyanag)Saroj PandeyNoch keine Bewertungen
- (PEDIA) Developmental ConditionsDokument8 Seiten(PEDIA) Developmental ConditionsPAULINE VIVIEN ACLANNoch keine Bewertungen
- Handbook of Childhood Developmental DisordersDokument20 SeitenHandbook of Childhood Developmental DisordersObiajuru Ikechukwu100% (1)
- Letter To The Editor: On Cognitive Variability in Velocardiofacial Syndrome: Profound Mental Retardation and AutismDokument2 SeitenLetter To The Editor: On Cognitive Variability in Velocardiofacial Syndrome: Profound Mental Retardation and AutismHarshit AmbeshNoch keine Bewertungen
- Journal Related To Neurodevelopmental DisordersDokument4 SeitenJournal Related To Neurodevelopmental DisordersRuchelle SemsemNoch keine Bewertungen
- Handouts in Special and Inclusive EducationDokument2 SeitenHandouts in Special and Inclusive EducationRex EvangelistaNoch keine Bewertungen
- Early Onset SchizophreniaDokument3 SeitenEarly Onset SchizophreniaDoc Prince CaballeroNoch keine Bewertungen
- Alzheimer's Disease: DementiaDokument18 SeitenAlzheimer's Disease: DementiaBerny VillavicencioNoch keine Bewertungen
- UMS Paediatric Short Cases Records 1st EditionDokument17 SeitenUMS Paediatric Short Cases Records 1st EditionHengkai NeoNoch keine Bewertungen
- SlideshowDokument19 SeitenSlideshowbelair1Noch keine Bewertungen
- Down Syndrome Power PointDokument28 SeitenDown Syndrome Power PointJamesNoch keine Bewertungen
- Mental RetardationDokument7 SeitenMental RetardationNikhil MohanNoch keine Bewertungen
- PWS, AgDokument12 SeitenPWS, Agmohadese.hnprNoch keine Bewertungen
- FINALLLDokument58 SeitenFINALLLImie AldoyesaNoch keine Bewertungen
- Communication Disorders in Psychiatric ConditionsDokument42 SeitenCommunication Disorders in Psychiatric Conditionsrsunilkumar86Noch keine Bewertungen
- An Overview of DementiaDokument44 SeitenAn Overview of DementiaAnil KakunjeNoch keine Bewertungen
- PsychiatryDokument20 SeitenPsychiatryAroosha IbrahimNoch keine Bewertungen
- Foundation of Inclusive and Special Education: Local Flavor. Global FutureDokument20 SeitenFoundation of Inclusive and Special Education: Local Flavor. Global FutureShai MacapillarNoch keine Bewertungen
- Types of DisabilitiesDokument24 SeitenTypes of DisabilitiesvicentemariscalNoch keine Bewertungen
- Week 11 Introduction To Philosophy of The Human PersonDokument7 SeitenWeek 11 Introduction To Philosophy of The Human PersonMarcel Baring ImperialNoch keine Bewertungen
- Intellectual Disability DisorderDokument63 SeitenIntellectual Disability DisorderRenz Ian RaroNoch keine Bewertungen
- A. DizabilitatiDokument73 SeitenA. DizabilitatiNia AdibNoch keine Bewertungen
- PotongDokument11 SeitenPotongmuatbanyak1000Noch keine Bewertungen
- A Simple Guide to Riley-Day Syndrome (Familial Dysautonomia), Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Riley-Day Syndrome (Familial Dysautonomia), Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Ordaneza - Autism Spectrum DisorderDokument84 SeitenOrdaneza - Autism Spectrum DisorderMA. ESPERANZA ORDANEZANoch keine Bewertungen
- Intellectual Disability With QuizDokument52 SeitenIntellectual Disability With QuizCarla Andrea QuilloNoch keine Bewertungen
- Nursing Care of The Older Patient in Chronic IllnessDokument40 SeitenNursing Care of The Older Patient in Chronic IllnessMaggay LarsNoch keine Bewertungen
- Introduction To Mental Health Care of People With Intellectual DisabilityDokument65 SeitenIntroduction To Mental Health Care of People With Intellectual DisabilityFrancois CreweNoch keine Bewertungen
- Lewy Body Dementia: Causes, Tests and Treatment OptionsVon EverandLewy Body Dementia: Causes, Tests and Treatment OptionsBewertung: 4 von 5 Sternen4/5 (1)
- Genetic Disorders Lec # 6Dokument43 SeitenGenetic Disorders Lec # 6MISS. COMNoch keine Bewertungen
- Minds Fading Away : Alzheimer's And Dementia GuideVon EverandMinds Fading Away : Alzheimer's And Dementia GuideBewertung: 5 von 5 Sternen5/5 (1)
- Q2 SLHT6Dokument13 SeitenQ2 SLHT6ALEX SARAOSOSNoch keine Bewertungen
- Mental RetardationDokument22 SeitenMental RetardationRobert Farrugia100% (1)
- Foundation of Inclusive and Special Education: Local Flavor. Global FutureDokument13 SeitenFoundation of Inclusive and Special Education: Local Flavor. Global FutureShai MacapillarNoch keine Bewertungen
- Genetic Disorders: U Me and SocietyDokument23 SeitenGenetic Disorders: U Me and SocietyDeepansh GuptaNoch keine Bewertungen
- Intro To Philo 2nd Monthly - BDokument35 SeitenIntro To Philo 2nd Monthly - BPrincess Shara CastroNoch keine Bewertungen
- Mental Retar.lDokument15 SeitenMental Retar.lwel2332Noch keine Bewertungen
- Navigating Lewy Body Dementia and Parkinson's Disease, A Comprehensive Guide from Diagnosis to TreatmentVon EverandNavigating Lewy Body Dementia and Parkinson's Disease, A Comprehensive Guide from Diagnosis to TreatmentNoch keine Bewertungen
- Shanz - Pedia 1.01Dokument7 SeitenShanz - Pedia 1.01Petrina XuNoch keine Bewertungen
- Sports BettingDokument2 SeitenSports Bettingapi-664323141Noch keine Bewertungen
- Mass Assault ManualDokument107 SeitenMass Assault ManualChak Puk Ram100% (6)
- Commonwealth GamesDokument6 SeitenCommonwealth GamesMahesh T MadhavanNoch keine Bewertungen
- Knole Run 11012014 Full ResultsDokument19 SeitenKnole Run 11012014 Full ResultsSpectrumNoch keine Bewertungen
- Horses and Sport: Horse Sport Within Current European PolicymakingDokument2 SeitenHorses and Sport: Horse Sport Within Current European PolicymakingOrientación Juan ReyNoch keine Bewertungen
- Pe 2ND QTR ReviewerDokument6 SeitenPe 2ND QTR ReviewerBeefWith PorkNoch keine Bewertungen
- Seksyen Math LatestDokument5 SeitenSeksyen Math LatestMazeta TormanNoch keine Bewertungen
- 2017 Arizona Hideaway Book PDFDokument109 Seiten2017 Arizona Hideaway Book PDFVanNoch keine Bewertungen
- What Is BADMINTONDokument1 SeiteWhat Is BADMINTONJoseph Neil TacataniNoch keine Bewertungen
- Osram HQI Power Stars Lamps BrochureDokument4 SeitenOsram HQI Power Stars Lamps BrochureAlan MastersNoch keine Bewertungen
- BODYATTACK 120 (BODYATTACK120ChoreographyNotes Row en App Print PDFDokument33 SeitenBODYATTACK 120 (BODYATTACK120ChoreographyNotes Row en App Print PDFpietraNoch keine Bewertungen
- The Relationshipbetween Ownership Structureand Club Performanceinthe EPLDokument19 SeitenThe Relationshipbetween Ownership Structureand Club Performanceinthe EPLCB19K069川名裕樹Noch keine Bewertungen
- Anatomy Flexibility and Joint LimitationsDokument22 SeitenAnatomy Flexibility and Joint LimitationsMichelle Echeverria100% (2)
- World Cup 2022Dokument3 SeitenWorld Cup 2022zulhaizadNoch keine Bewertungen
- 2019 Southeast Asian Games Cauldron PDFDokument2 Seiten2019 Southeast Asian Games Cauldron PDFPatricia Camille Nepomuceno MateoNoch keine Bewertungen
- CapitalizationDokument2 SeitenCapitalizationJen Ni Fer100% (1)
- Week5 6 2Dokument2 SeitenWeek5 6 2SAMANIEGO BERMEO DAVID SEBASTIANNoch keine Bewertungen
- Section A Short Story: How Noah Discovered A Magical LandDokument8 SeitenSection A Short Story: How Noah Discovered A Magical LandviniNoch keine Bewertungen
- Pareto Chart: Basic Tools For Process ImprovementDokument49 SeitenPareto Chart: Basic Tools For Process ImprovementGirish RajNoch keine Bewertungen
- Elite Women's XCO: 2018 UCI Mountain Bike World Championships - Lenzerheide, SwitzerlandDokument2 SeitenElite Women's XCO: 2018 UCI Mountain Bike World Championships - Lenzerheide, SwitzerlandMatthew PioroNoch keine Bewertungen
- Cardiovascular Physical ExaminationDokument45 SeitenCardiovascular Physical Examinationrosita100% (1)
- Answers: Short TextsDokument4 SeitenAnswers: Short TextsYashini BubalanNoch keine Bewertungen
- Bikes List PDFDokument3 SeitenBikes List PDFNehal RaiNoch keine Bewertungen
- Aerodynamics in Formula 1 Racing 2 2Dokument6 SeitenAerodynamics in Formula 1 Racing 2 2api-390681562Noch keine Bewertungen
- Palawanseaexplorer CV-PortfolioDokument3 SeitenPalawanseaexplorer CV-PortfolioBen RiverNoch keine Bewertungen
- Past and Projected Future Overweight Rates in Selected OECD CountriesDokument17 SeitenPast and Projected Future Overweight Rates in Selected OECD CountriesEvariste ZephyrinNoch keine Bewertungen
- Ulhar B.ing Kelas 6 by Ms. Rahma Hidayatus S.Dokument2 SeitenUlhar B.ing Kelas 6 by Ms. Rahma Hidayatus S.Afifudin HidayatullahNoch keine Bewertungen
- The 10 Year Rule Has Been KnownDokument2 SeitenThe 10 Year Rule Has Been Knownapi-26661807Noch keine Bewertungen
- Versys 650 E-BrochureDokument1 SeiteVersys 650 E-Brochureanip_5903Noch keine Bewertungen
- Adidas Case StudyDokument14 SeitenAdidas Case StudyMehatab NabiNoch keine Bewertungen