Das könnte Ihnen auch gefallen
- Kenya Asthma Management GuidelineDokument124 SeitenKenya Asthma Management Guidelinewhoosh2008Noch keine Bewertungen
- FGH 2019 Interior Final Online 2020.09.18Dokument180 SeitenFGH 2019 Interior Final Online 2020.09.18whoosh2008Noch keine Bewertungen
- Case - Liberia Case Study, Leadership and Policy DevelopmentDokument10 SeitenCase - Liberia Case Study, Leadership and Policy Developmentwhoosh2008Noch keine Bewertungen
- Building Effective Public-Private Collaboration in HealthcareDokument88 SeitenBuilding Effective Public-Private Collaboration in Healthcarewhoosh2008Noch keine Bewertungen
- FGH 2019 Interior Final Online 2020.09.18Dokument180 SeitenFGH 2019 Interior Final Online 2020.09.18whoosh2008Noch keine Bewertungen
- Cringoli Et Al - Nat Protoc (9 - 2017)Dokument10 SeitenCringoli Et Al - Nat Protoc (9 - 2017)whoosh2008Noch keine Bewertungen
- Interim MNGMT Guide For Covid19 - and TBDokument62 SeitenInterim MNGMT Guide For Covid19 - and TBwhoosh2008Noch keine Bewertungen
- PPM Action Plan - 13 - 01 - 2022Dokument128 SeitenPPM Action Plan - 13 - 01 - 2022whoosh2008Noch keine Bewertungen
- Kenya Health Financing Strategy 2020–2030Dokument85 SeitenKenya Health Financing Strategy 2020–2030whoosh2008Noch keine Bewertungen
- Gebre Lancet 122111Dokument9 SeitenGebre Lancet 122111whoosh2008Noch keine Bewertungen
- WHO AF WHE CPI 05.2019 Eng PDFDokument77 SeitenWHO AF WHE CPI 05.2019 Eng PDFwilliam foday moiforayNoch keine Bewertungen
- Kenya Health Survey Reveals Household Spending TrendsDokument103 SeitenKenya Health Survey Reveals Household Spending Trendswhoosh2008Noch keine Bewertungen
- Costs of UHC - Working Paper - Watkins - Final 13 Nov - 0Dokument30 SeitenCosts of UHC - Working Paper - Watkins - Final 13 Nov - 0whoosh2008Noch keine Bewertungen
- WHO AF WHE CPI 05.2019 Eng PDFDokument77 SeitenWHO AF WHE CPI 05.2019 Eng PDFwilliam foday moiforayNoch keine Bewertungen
- Community Wide Cross Sectional SurveyDokument9 SeitenCommunity Wide Cross Sectional Surveywhoosh2008Noch keine Bewertungen
- Epidemiological Characteristics of C19 in KenyaDokument21 SeitenEpidemiological Characteristics of C19 in Kenyawhoosh2008Noch keine Bewertungen
- Econometrics: Autocorrelation: What Happens If The Error Terms Are Correlated?Dokument43 SeitenEconometrics: Autocorrelation: What Happens If The Error Terms Are Correlated?whoosh2008Noch keine Bewertungen
- Insead Knowledge Eight Key Points of Blue Ocean Strategy PDFDokument3 SeitenInsead Knowledge Eight Key Points of Blue Ocean Strategy PDFrehanNoch keine Bewertungen
- Multiple Regression Analysis, The Problem of EstimationDokument53 SeitenMultiple Regression Analysis, The Problem of Estimationwhoosh2008Noch keine Bewertungen
- Econometrics: Multicollinearity: What Happens If The Regressors Are Correlated?Dokument45 SeitenEconometrics: Multicollinearity: What Happens If The Regressors Are Correlated?whoosh2008Noch keine Bewertungen
- Nature of Regression AnalysisDokument22 SeitenNature of Regression Analysiswhoosh2008Noch keine Bewertungen
- Two-Variable Regression Analysis BasicsDokument28 SeitenTwo-Variable Regression Analysis Basicswhoosh2008Noch keine Bewertungen
- 1 IntroductionDokument19 Seiten1 Introductionwhoosh2008Noch keine Bewertungen
- Econometrics: Two-Variable Regression Interval Estimation and Hypothesis TestingDokument51 SeitenEconometrics: Two-Variable Regression Interval Estimation and Hypothesis Testingwhoosh2008Noch keine Bewertungen
- Two-Variable Regression Model, The Problem of EstimationDokument67 SeitenTwo-Variable Regression Model, The Problem of Estimationwhoosh2008Noch keine Bewertungen
- Classical Normal Linear Regression ModelDokument13 SeitenClassical Normal Linear Regression Modelwhoosh2008Noch keine Bewertungen
- Econometrics: Two-Variable Regression Interval Estimation and Hypothesis TestingDokument51 SeitenEconometrics: Two-Variable Regression Interval Estimation and Hypothesis Testingwhoosh2008Noch keine Bewertungen
- Two-Variable Regression Model, The Problem of EstimationDokument67 SeitenTwo-Variable Regression Model, The Problem of Estimationwhoosh2008Noch keine Bewertungen
- Classical Normal Linear Regression ModelDokument13 SeitenClassical Normal Linear Regression Modelwhoosh2008Noch keine Bewertungen
- Two-Variable Regression Analysis BasicsDokument28 SeitenTwo-Variable Regression Analysis Basicswhoosh2008Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Common Viral Infections Including Corona (Covid Infection) in Children - A ReviewDokument10 SeitenCommon Viral Infections Including Corona (Covid Infection) in Children - A ReviewIJAR JOURNALNoch keine Bewertungen
- Maternal Immunological Adaptation During Normal PregnancyDokument20 SeitenMaternal Immunological Adaptation During Normal PregnancyANDRÉS FELIPE BUSTILLO GÓMEZNoch keine Bewertungen
- The Effect of Inflammation On BoneDokument14 SeitenThe Effect of Inflammation On BoneKelas CNoch keine Bewertungen
- Rational Use of BloodDokument21 SeitenRational Use of BloodAllan MacacapagalNoch keine Bewertungen
- Contact DermatitisDokument70 SeitenContact DermatitisThariq Mubaraq DrcNoch keine Bewertungen
- Plot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015Dokument3 SeitenPlot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015Asit ANoch keine Bewertungen
- Argument Essay ReflectionDokument5 SeitenArgument Essay Reflectionapi-509671089Noch keine Bewertungen
- Human MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyDokument34 SeitenHuman MAIT Cells Are Devoid of Alloreactive Potential: Prompting Their Use As Universal Cells For Adoptive Immune TherapyJános JuhászNoch keine Bewertungen
- Pregnant Healthcare Personnel - Infection Prevention For Occupational Health - Table of Contents - APICDokument35 SeitenPregnant Healthcare Personnel - Infection Prevention For Occupational Health - Table of Contents - APICsalamon2tNoch keine Bewertungen
- Evidence Based Practice On Typhoid FeverDokument22 SeitenEvidence Based Practice On Typhoid FeverRhia CortezNoch keine Bewertungen
- PATIENT RECORDSDokument19 SeitenPATIENT RECORDSRieWibawaNoch keine Bewertungen
- Prevention and Control of Diseases and DisordersDokument45 SeitenPrevention and Control of Diseases and DisordersBhel San Pedro MarzanNoch keine Bewertungen
- 080001Dokument21 Seiten080001Pearl MayNoch keine Bewertungen
- Urinary System Test BankDokument30 SeitenUrinary System Test BankVinz TombocNoch keine Bewertungen
- 7.2. Hemolytic AnemiaDokument29 Seiten7.2. Hemolytic AnemiaMichellyTjoaNoch keine Bewertungen
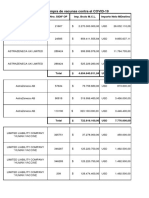
- Pagos Efectuados A LaboratoriosDokument14 SeitenPagos Efectuados A LaboratoriosCronista.comNoch keine Bewertungen
- 5.2 PhysDokument39 Seiten5.2 PhysshivaniNoch keine Bewertungen
- Module 1 - TransDokument8 SeitenModule 1 - TransJohanna Kate DiestroNoch keine Bewertungen
- Diagnosis BandingDokument5 SeitenDiagnosis BandingMuhammad Hafiz IINoch keine Bewertungen
- Micropara Open BookDokument2 SeitenMicropara Open BookAlahrick CorpuzNoch keine Bewertungen
- 5 Benefits of BoswelliaDokument6 Seiten5 Benefits of BoswelliaPaulNoch keine Bewertungen
- ReportsDokument5 SeitenReportsguptaaarushi528Noch keine Bewertungen
- Needle Prick InjuryDokument20 SeitenNeedle Prick InjuryThirugnanaThiruNoch keine Bewertungen
- Yanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalityDokument1 SeiteYanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalitylisaNoch keine Bewertungen
- Germ Crossword 2Dokument2 SeitenGerm Crossword 2Laura CotsNoch keine Bewertungen
- Cytokines - IntroductionDokument2 SeitenCytokines - IntroductionTra gicNoch keine Bewertungen
- Interpretations of SARS-CoV-2 IgM and IgG Antibody Titers in TheDokument7 SeitenInterpretations of SARS-CoV-2 IgM and IgG Antibody Titers in TheYunita AnggrainiNoch keine Bewertungen
- Risk Factors For Pneumonia in NeonatesDokument20 SeitenRisk Factors For Pneumonia in NeonatesPaula Andrea Perdomo SalamancaNoch keine Bewertungen
- Open Vial Policy - MoHFW - Sep2015Dokument6 SeitenOpen Vial Policy - MoHFW - Sep2015SaumyaNoch keine Bewertungen
- Reducing Malaria Infections in Sub-Saharan AfricaDokument2 SeitenReducing Malaria Infections in Sub-Saharan AfricaStansa SeniaNoch keine Bewertungen