Das könnte Ihnen auch gefallen
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- OtosclerosisDokument31 SeitenOtosclerosisashry909100% (1)
- Otosclerosis & Acostic NeuromaDokument44 SeitenOtosclerosis & Acostic NeuromaAbdullah AnsarNoch keine Bewertungen
- OtosclerosisDokument9 SeitenOtosclerosisHelgaNoch keine Bewertungen
- O To SclerosisDokument9 SeitenO To SclerosisHelgaNoch keine Bewertungen
- Background: MeningitisDokument7 SeitenBackground: MeningitisranmiNoch keine Bewertungen
- Otosclerosis: Aditya Ghosh Roy PGT-2 M.S. E.N.T. N.R.S.M.C.HDokument130 SeitenOtosclerosis: Aditya Ghosh Roy PGT-2 M.S. E.N.T. N.R.S.M.C.Hanon_205487480Noch keine Bewertungen
- OTOSCLEROSISDokument75 SeitenOTOSCLEROSISShivaam KesarwaaniNoch keine Bewertungen
- Pediatric - Hearing - Loss Lau 3-17-10Dokument45 SeitenPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNoch keine Bewertungen
- Otosclerosis: Pathogenesis & ManagementDokument112 SeitenOtosclerosis: Pathogenesis & Managementanon_205487480Noch keine Bewertungen
- OtosclerosisDokument8 SeitenOtosclerosisAhlam DreamsNoch keine Bewertungen
- Chapter 143: Otosclerosis (OS) : Sameer Ahmed 2/23/2011Dokument20 SeitenChapter 143: Otosclerosis (OS) : Sameer Ahmed 2/23/2011Bedo BodyNoch keine Bewertungen
- Otosclerosis Presentation MBBSDokument119 SeitenOtosclerosis Presentation MBBSFaltuNoch keine Bewertungen
- Meniere's DiseaseDokument50 SeitenMeniere's DiseaseRaisa CleizeraNoch keine Bewertungen
- Otosclerosis Slides 061018Dokument96 SeitenOtosclerosis Slides 061018Paraguay De La Cruz JoelNoch keine Bewertungen
- OtosclerosisDokument31 SeitenOtosclerosisSubramaniyanNoch keine Bewertungen
- Otosclerosis Anddysplasias of Thetemporal BoneDokument19 SeitenOtosclerosis Anddysplasias of Thetemporal BoneDianithus169Noch keine Bewertungen
- Conductive Hearing Loss With An Intact Tympanic Membrane: Diagnosed ApproachesDokument5 SeitenConductive Hearing Loss With An Intact Tympanic Membrane: Diagnosed ApproachesMonika ZikraNoch keine Bewertungen
- OTOSCLEROSISDokument21 SeitenOTOSCLEROSISmounikaNoch keine Bewertungen
- Batson2017 OtosclerosisDokument6 SeitenBatson2017 OtosclerosisnuhajazminNoch keine Bewertungen
- CR Couzon SyndromeDokument3 SeitenCR Couzon SyndromeDevi RistikaNoch keine Bewertungen
- Seminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M LuxonDokument9 SeitenSeminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M Luxonmaria_garaveNoch keine Bewertungen
- O To SclerosisDokument23 SeitenO To SclerosisJennifer Dixon100% (1)
- OtosclerosisDokument9 SeitenOtosclerosisSuprit SnNoch keine Bewertungen
- Sensorineural Hearing LossDokument19 SeitenSensorineural Hearing LossBenitaNoch keine Bewertungen
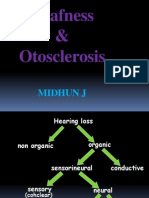
- Deafness & Otosclerosis: Midhun JDokument44 SeitenDeafness & Otosclerosis: Midhun JRohit R PillaiNoch keine Bewertungen
- OTOSCLEROSISDokument75 SeitenOTOSCLEROSISShivaam KesarwaaniNoch keine Bewertungen
- Otosclerosis Content PDFDokument12 SeitenOtosclerosis Content PDFAhmed MorsyNoch keine Bewertungen
- Perthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore PakistanDokument68 SeitenPerthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore Pakistandrakkashmiri50% (2)
- Current Care and Investigational Therapies in AchondroplasiaDokument8 SeitenCurrent Care and Investigational Therapies in Achondroplasiachristian roblesNoch keine Bewertungen
- Matsy CytoDokument7 SeitenMatsy CytoDarem SoNoch keine Bewertungen
- Final PottsDokument60 SeitenFinal Pottsharsh.chandane100% (6)
- Vertigo: A Review of Common Peripheral and Central Vestibular DisordersDokument7 SeitenVertigo: A Review of Common Peripheral and Central Vestibular DisordersPutra ImanullahNoch keine Bewertungen
- Choanal Atresia2Dokument40 SeitenChoanal Atresia2pramod555Noch keine Bewertungen
- Diseases and TreatmentDokument42 SeitenDiseases and Treatmentheena solankiNoch keine Bewertungen
- Nikolaus Ronald Indra 4Dokument137 SeitenNikolaus Ronald Indra 4Florence StellaNoch keine Bewertungen
- Study of The Disease AchondraplasiaDokument5 SeitenStudy of The Disease AchondraplasiaEries Lacanlale LumbaNoch keine Bewertungen
- Pedi HN SlidesDokument71 SeitenPedi HN SlidesvelangniNoch keine Bewertungen
- Холестериновая гранулемаDokument13 SeitenХолестериновая гранулемаНатальяNoch keine Bewertungen
- Meniere's Disease & OtosclerosisDokument44 SeitenMeniere's Disease & OtosclerosisNadzirah Ahmad JailaniNoch keine Bewertungen
- Sdarticle PDFDokument9 SeitenSdarticle PDFManjeev GuragainNoch keine Bewertungen
- The Medical Treatment of Otosclerosis 20100730Dokument42 SeitenThe Medical Treatment of Otosclerosis 20100730shibhiNoch keine Bewertungen
- Otosclerosis LT11 KHDokument57 SeitenOtosclerosis LT11 KHKyaw HtetNoch keine Bewertungen
- Silent Sinus Syndrome: An Acquired Condition: Case ReportDokument3 SeitenSilent Sinus Syndrome: An Acquired Condition: Case Reportbdalcin5512Noch keine Bewertungen
- Tuli Mendadak (Sudden Deafness)Dokument26 SeitenTuli Mendadak (Sudden Deafness)Marisa FatkiyaNoch keine Bewertungen
- Oto TemporalDokument13 SeitenOto TemporalMoisés AarónNoch keine Bewertungen
- Sordera SindromicaDokument8 SeitenSordera SindromicaFabian Camelo OtorrinoNoch keine Bewertungen
- Jurnal Tamara AsliDokument5 SeitenJurnal Tamara AsliYohanaNoch keine Bewertungen
- Cochlear OtosclerosisDokument6 SeitenCochlear OtosclerosisadriricaldeNoch keine Bewertungen
- Word HereditereyDokument7 SeitenWord Hereditereypxb8dhqgs9Noch keine Bewertungen
- Drtbalu'S Otolaryngology Online: PresbyacusisDokument3 SeitenDrtbalu'S Otolaryngology Online: PresbyacusisAnish RajNoch keine Bewertungen
- Cholesteatoma of External Auditory CanalDokument5 SeitenCholesteatoma of External Auditory CanallolNoch keine Bewertungen
- Choanal Atresia2Dokument40 SeitenChoanal Atresia2Mavina ReeNaNoch keine Bewertungen
- Jurnal-NCBI-Paralisis Korda VokalisDokument20 SeitenJurnal-NCBI-Paralisis Korda VokalisAchmad Hafidz BaraqbahNoch keine Bewertungen
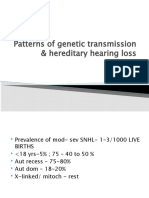
- Patterns of Genetic Transmission & Hereditary Hearing Loss: DR - DivyaDokument60 SeitenPatterns of Genetic Transmission & Hereditary Hearing Loss: DR - DivyavipinNoch keine Bewertungen
- J Risk Factr PDFDokument4 SeitenJ Risk Factr PDFdevyNoch keine Bewertungen
- Orthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsVon EverandOrthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsSu-Jung KimNoch keine Bewertungen
- Amplivox CA 850-2 ManualDokument55 SeitenAmplivox CA 850-2 ManualPraistonNoch keine Bewertungen
- Approach To Hearing LossDokument7 SeitenApproach To Hearing LossAlexandros GidarakosNoch keine Bewertungen
- Rangifer Tarandus Tarandus) Perception of Noise From Power LinesDokument4 SeitenRangifer Tarandus Tarandus) Perception of Noise From Power LinesAzalia BakhtiarNoch keine Bewertungen
- Instructions For Use Diagnostic Suite UsDokument47 SeitenInstructions For Use Diagnostic Suite UszeroseyaNoch keine Bewertungen
- GATIOD Fifth Edition Disability CalculatiionDokument90 SeitenGATIOD Fifth Edition Disability CalculatiionMarco Antonio Borges das NevesNoch keine Bewertungen
- Audiometry Screening and InterpretationDokument8 SeitenAudiometry Screening and InterpretationJuan Sebastián Montaño MaldonadoNoch keine Bewertungen
- MA 53 Operating InstructionsDokument53 SeitenMA 53 Operating InstructionsALEXANDER1819Noch keine Bewertungen
- Hearing Loss AssessmentDokument31 SeitenHearing Loss AssessmentKIBET ERNEST MUTAINoch keine Bewertungen
- Back To Basics - Speech Audiometry Janet RDokument7 SeitenBack To Basics - Speech Audiometry Janet RBrett RodriguezNoch keine Bewertungen
- AudiometryDokument2 SeitenAudiometryRajesh ChundiNoch keine Bewertungen
- Welch Allyn® AM282 Auto Tymp: Part Number 28204 Rev GDokument36 SeitenWelch Allyn® AM282 Auto Tymp: Part Number 28204 Rev GJuan PáezNoch keine Bewertungen
- Otosclerosis An Update On Diagnosis and Treatment.3Dokument6 SeitenOtosclerosis An Update On Diagnosis and Treatment.3andiNoch keine Bewertungen
- The Bloomsbury Handbook of Sonic Methodologies by Michael Bull and Marcel CobussenDokument849 SeitenThe Bloomsbury Handbook of Sonic Methodologies by Michael Bull and Marcel CobussenLuis Fernando Muniz CirneNoch keine Bewertungen
- Hearing Conservation ManualDokument28 SeitenHearing Conservation ManualEbru EvranNoch keine Bewertungen
- Operating Manual Audiometry ModuleDokument30 SeitenOperating Manual Audiometry ModuleJuan Carlos Enríquez GómezNoch keine Bewertungen
- ENT Lecture NotesDokument190 SeitenENT Lecture NotesMizrab NadeemNoch keine Bewertungen
- Reference Manual Itera IIDokument134 SeitenReference Manual Itera IIEdson Davi SantanaNoch keine Bewertungen
- FMA RegsDokument361 SeitenFMA RegsJiong SoonNoch keine Bewertungen
- AUDIOMETERDokument11 SeitenAUDIOMETERYogesh PolNoch keine Bewertungen
- Behavioural Observation AudiometryDokument4 SeitenBehavioural Observation AudiometryLubaba lubinpNoch keine Bewertungen
- Audiometers OK PDFDokument81 SeitenAudiometers OK PDFErnesto AcostaNoch keine Bewertungen
- HP502 OSHA Amendment Poster 002Dokument1 SeiteHP502 OSHA Amendment Poster 002NorthNoch keine Bewertungen
- Sa201 IvDokument2 SeitenSa201 IvsermedNoch keine Bewertungen
- 6-PL Approved Notification With Annexture-V - 042023 - 210423Dokument44 Seiten6-PL Approved Notification With Annexture-V - 042023 - 210423Sid MadishettyNoch keine Bewertungen
- 12 Audiometic TestingDokument99 Seiten12 Audiometic TestingAashish SinghNoch keine Bewertungen
- New Count The DotsDokument1 SeiteNew Count The Dotslin ee100% (1)
- 3.0 - Occupational Noise v3.0 EnglishDokument22 Seiten3.0 - Occupational Noise v3.0 EnglishkapilNoch keine Bewertungen
- AudiometryDokument3 SeitenAudiometrySathish KumarNoch keine Bewertungen
- Amplivox PC850 Operating ManualDokument33 SeitenAmplivox PC850 Operating ManualmacrufoNoch keine Bewertungen
- Oscilla - Excellence Since 1960Dokument24 SeitenOscilla - Excellence Since 1960Pau Choon HockNoch keine Bewertungen