Das könnte Ihnen auch gefallen
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsVon EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNoch keine Bewertungen
- Rehabilitation Hospice and Palliative CareDokument20 SeitenRehabilitation Hospice and Palliative CarePaul Bryan SanchezNoch keine Bewertungen
- Case Management 101Dokument51 SeitenCase Management 101bulatyNoch keine Bewertungen
- Cost Effective Home Care in MassachusettsDokument25 SeitenCost Effective Home Care in MassachusettsTom MeyerNoch keine Bewertungen
- Permj18 2p0077Dokument9 SeitenPermj18 2p0077Vaishnavi AgrawalNoch keine Bewertungen
- Palliative CareDokument34 SeitenPalliative CareSandy ShahNoch keine Bewertungen
- Palliative Medicine and Supportive CareDokument12 SeitenPalliative Medicine and Supportive CareKaren CárcamoNoch keine Bewertungen
- SN VisitDokument8 SeitenSN VisiteleahtNoch keine Bewertungen
- Home Health Care and Diabetes Assessment, Care, and EducationDokument4 SeitenHome Health Care and Diabetes Assessment, Care, and EducationKundan KumarNoch keine Bewertungen
- Unit 2-Community Health Nursing Roles (Autosaved)Dokument57 SeitenUnit 2-Community Health Nursing Roles (Autosaved)Krista KloseNoch keine Bewertungen
- Congestive Heart Failure: Caroline L. Guglielmetti RN, BSNDokument19 SeitenCongestive Heart Failure: Caroline L. Guglielmetti RN, BSNbudoy00Noch keine Bewertungen
- Palliative Care Assignment.Dokument6 SeitenPalliative Care Assignment.NATHANIEL YERINoch keine Bewertungen
- Chronic Illness Acute Illness: CharacteristicsDokument4 SeitenChronic Illness Acute Illness: CharacteristicsFerdinand Sherwin MorataNoch keine Bewertungen
- Lecture #7, Points On The Continuum - Ambulatory Care, Home Care, Hospice and Palliative CareDokument17 SeitenLecture #7, Points On The Continuum - Ambulatory Care, Home Care, Hospice and Palliative CareKathleen LaNoch keine Bewertungen
- Does You Patient Meet Medicare Homebound Criteria?: Stop NO ReferralDokument1 SeiteDoes You Patient Meet Medicare Homebound Criteria?: Stop NO ReferralMukulDabasNoch keine Bewertungen
- Hospital Admission and DischargeDokument21 SeitenHospital Admission and DischargeYogesh ChandraNoch keine Bewertungen
- Revised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)Dokument6 SeitenRevised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)NATHANIEL YERINoch keine Bewertungen
- Transition of CareDokument7 SeitenTransition of CareJisna Alby100% (1)
- 1 IntroductionDokument4 Seiten1 IntroductionRajih AbdulwasiNoch keine Bewertungen
- Fam MedicineDokument18 SeitenFam MedicineAbubakar JallohNoch keine Bewertungen
- l1 Introduction To Family Medicine.Dokument33 Seitenl1 Introduction To Family Medicine.Shidev50% (4)
- CGA Deeds StudyDokument7 SeitenCGA Deeds StudyNatanNoch keine Bewertungen
- Referral SystemDokument3 SeitenReferral SystemHannah aswini100% (1)
- Hospice CareDokument7 SeitenHospice CareJason SteelNoch keine Bewertungen
- Running Head: QSEN 1Dokument11 SeitenRunning Head: QSEN 1Mariam AbedNoch keine Bewertungen
- End of Life CareDokument22 SeitenEnd of Life CareMkindiNoch keine Bewertungen
- Care Plan 1 240Dokument16 SeitenCare Plan 1 240api-314575117Noch keine Bewertungen
- Admission and Discharge Resource MaterialDokument13 SeitenAdmission and Discharge Resource MaterialCherry Louise O. SanvictoresNoch keine Bewertungen
- Pelayanan PaliatifDokument43 SeitenPelayanan PaliatifBety RindaNoch keine Bewertungen
- Factors Affecting Health and IllnessDokument5 SeitenFactors Affecting Health and IllnessVanessa Mae IlaganNoch keine Bewertungen
- Discharge PlanningDokument28 SeitenDischarge PlanningkrgduraiNoch keine Bewertungen
- This Is To Be A Detailed Plan Using The METHOD-P Format. It Is To Be Written With Each AreaDokument3 SeitenThis Is To Be A Detailed Plan Using The METHOD-P Format. It Is To Be Written With Each AreaMia Paloma LawsonNoch keine Bewertungen
- DISCHARGE PLANNING & REFERRALS STUDENT VIEW-revised 2-6-16Dokument41 SeitenDISCHARGE PLANNING & REFERRALS STUDENT VIEW-revised 2-6-16Julia Andreigna LAGCAONoch keine Bewertungen
- Msii Pat 2Dokument22 SeitenMsii Pat 2api-300946501Noch keine Bewertungen
- End of Life Care For Nurses DMH FinalDokument39 SeitenEnd of Life Care For Nurses DMH FinalpradeepNoch keine Bewertungen
- Palliative Care in IcuDokument74 SeitenPalliative Care in IcupradeepNoch keine Bewertungen
- The Yale Way - New Patient PresentationsDokument9 SeitenThe Yale Way - New Patient PresentationsAndrew McGowanNoch keine Bewertungen
- Home Visits A PrimerDokument50 SeitenHome Visits A PrimerFika FathiaNoch keine Bewertungen
- Home Care and Family PhysicianDokument25 SeitenHome Care and Family PhysicianHanif Alienda WardhaniNoch keine Bewertungen
- Access To Palliative Care and Hospice in Nursing HomesDokument6 SeitenAccess To Palliative Care and Hospice in Nursing HomesfiennesrnNoch keine Bewertungen
- Nursing Care PlanDokument16 SeitenNursing Care PlanJennifer Post100% (3)
- Healthcare Training DocumentDokument50 SeitenHealthcare Training Documentdeeptimayeebarik6Noch keine Bewertungen
- Hospital Admission To Discharge 13 3 12 OkDokument3 SeitenHospital Admission To Discharge 13 3 12 OkHarry Wahyudhy UtamaNoch keine Bewertungen
- Advance Care Planning-Malaysian Hospice Congress - DR Wu Huei YawDokument42 SeitenAdvance Care Planning-Malaysian Hospice Congress - DR Wu Huei Yawmalaysianhospicecouncil6240Noch keine Bewertungen
- Nursing Care PlanDokument16 SeitenNursing Care PlanMelody B. MiguelNoch keine Bewertungen
- Chronic Disease - Treatment at HomeDokument77 SeitenChronic Disease - Treatment at HomeAmalNoch keine Bewertungen
- Ref 25 PDFDokument4 SeitenRef 25 PDFMuhammadIrsyadatNoch keine Bewertungen
- Danielle Doberman Geriatric Palliative CareDokument46 SeitenDanielle Doberman Geriatric Palliative CareArsya WinaNoch keine Bewertungen
- Trends in Maternal and Child CareDokument24 SeitenTrends in Maternal and Child CareJose Richard Giray100% (1)
- Review Process of Discharge Planning: by Janet BowenDokument11 SeitenReview Process of Discharge Planning: by Janet BowenAfiatur RohimahNoch keine Bewertungen
- End of Life, Palliative CareDokument35 SeitenEnd of Life, Palliative CareFranz TariganNoch keine Bewertungen
- Discharge PlaningDokument28 SeitenDischarge PlaningRuhiyat Spd100% (1)
- Role of Observational Medicine in EmergencyDokument13 SeitenRole of Observational Medicine in EmergencyazhaabazNoch keine Bewertungen
- Utilization Review RNDokument2 SeitenUtilization Review RNapi-121451258Noch keine Bewertungen
- PT SafetyDokument9 SeitenPT Safetyabaidurrehman0546Noch keine Bewertungen
- Referral ProcessDokument6 SeitenReferral ProcessCommunity BNoch keine Bewertungen
- Ambulatory Care Medical Surgical NursingDokument11 SeitenAmbulatory Care Medical Surgical NursingNiña Antoniette Gutang100% (4)
- Latecia 2023 ResumeDokument6 SeitenLatecia 2023 Resumeapi-643213493Noch keine Bewertungen
- The Business Case To Care For Persons With Serious.9Dokument7 SeitenThe Business Case To Care For Persons With Serious.9enfaraujoNoch keine Bewertungen
- ROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)Dokument45 SeitenROJOSON-PEP-TALK: Home Management of COVID19 Patient (May 22, 2021)rojosonNoch keine Bewertungen
- Recipes From Different SourcesDokument26 SeitenRecipes From Different SourcesCharisse Nicole DiazNoch keine Bewertungen
- Prayer To Saint HannibalDokument3 SeitenPrayer To Saint HannibalCharisse Nicole DiazNoch keine Bewertungen
- Module 3Dokument4 SeitenModule 3Charisse Nicole DiazNoch keine Bewertungen
- Bof Ost ListDokument1 SeiteBof Ost ListCharisse Nicole DiazNoch keine Bewertungen
- CHED MEMORANDUM ORDER (CMO) No. 14 Series of 2009Dokument129 SeitenCHED MEMORANDUM ORDER (CMO) No. 14 Series of 2009lylesantos85% (48)
- Burger Steak Jollibee StyleDokument2 SeitenBurger Steak Jollibee StyleCharisse Nicole DiazNoch keine Bewertungen
- Critical Response PaperDokument5 SeitenCritical Response PaperRomulux DoctoleroNoch keine Bewertungen
- Study Guide For TeachersDokument28 SeitenStudy Guide For TeachersHajar_Mzughi100% (1)
- Au Notes Act IIDokument3 SeitenAu Notes Act IICharisse Nicole DiazNoch keine Bewertungen
- Hypersensitivity PneumonitisDokument4 SeitenHypersensitivity PneumonitisCharisse Nicole DiazNoch keine Bewertungen
- Death of A Salesman Essay TopicsDokument3 SeitenDeath of A Salesman Essay TopicsCharisse Nicole DiazNoch keine Bewertungen
- Death of A Salesman Essay TopicsDokument3 SeitenDeath of A Salesman Essay TopicsCharisse Nicole DiazNoch keine Bewertungen
- Peplau's Interpersonal Relations Theory Power PointDokument10 SeitenPeplau's Interpersonal Relations Theory Power PointCharisse Nicole DiazNoch keine Bewertungen
- Peplau's Interpersonal Relations Theory Power PointDokument10 SeitenPeplau's Interpersonal Relations Theory Power PointCharisse Nicole DiazNoch keine Bewertungen
- Calc Drip Rates 2Dokument2 SeitenCalc Drip Rates 2Charisse Nicole DiazNoch keine Bewertungen
- Typhoid FeverDokument1 SeiteTyphoid FeverMarkChesterSaguidNagen100% (1)
- Hypersensitivity PneumonitisDokument4 SeitenHypersensitivity PneumonitisCharisse Nicole DiazNoch keine Bewertungen
- Big Mama - Winter ChildDokument6 SeitenBig Mama - Winter ChildNita CheamNoch keine Bewertungen
- Fluid and ElectrolytesDokument31 SeitenFluid and ElectrolytesCharisse Nicole DiazNoch keine Bewertungen
- Typhoid FeverDokument1 SeiteTyphoid FeverMarkChesterSaguidNagen100% (1)
- PediatricAPTA FactSheet PhysicalTherapistsPractitionerofChoice - 2020Dokument5 SeitenPediatricAPTA FactSheet PhysicalTherapistsPractitionerofChoice - 2020Juan Ignacio Gómez IruretagoyenaNoch keine Bewertungen
- Submitted To: The Chairman & MD,: CSR ProjectDokument14 SeitenSubmitted To: The Chairman & MD,: CSR ProjectsandeepNoch keine Bewertungen
- WillyRW PFP CSM 2019 PostedDokument29 SeitenWillyRW PFP CSM 2019 PostedRizky Meilynno CrisvantiknoNoch keine Bewertungen
- Security Supervisor 2. PhysiotherapistDokument4 SeitenSecurity Supervisor 2. PhysiotherapistJeshiNoch keine Bewertungen
- Nds Lower Quarter Course Manual PDFDokument105 SeitenNds Lower Quarter Course Manual PDFMskola Karlovac100% (1)
- Annual Report FY March 2012 (EXTRA INFO)Dokument212 SeitenAnnual Report FY March 2012 (EXTRA INFO)tangentssolNoch keine Bewertungen
- Rikta 04 4 Treatment Manual EngDokument211 SeitenRikta 04 4 Treatment Manual EngZvonko ŠuljakNoch keine Bewertungen
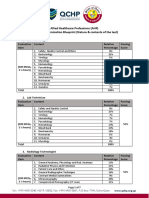
- AHP - Blueprint and Reference PDFDokument7 SeitenAHP - Blueprint and Reference PDFJashim JumliNoch keine Bewertungen
- Form B Allied ParticularsDokument26 SeitenForm B Allied ParticularsAravind RaviNoch keine Bewertungen
- Agreement For Physiotherapy Outsourcing Contract G.D. HospitalDokument4 SeitenAgreement For Physiotherapy Outsourcing Contract G.D. HospitalDebdoot BhattacharyaNoch keine Bewertungen
- Community Health Nursing Final Exam (Total Marks 80) I-Choose The Best Answers: - (25 Marks)Dokument10 SeitenCommunity Health Nursing Final Exam (Total Marks 80) I-Choose The Best Answers: - (25 Marks)Sukumari ImmadiNoch keine Bewertungen
- Rehabilitation Science and Disability Studies: Are They Complementary?Dokument23 SeitenRehabilitation Science and Disability Studies: Are They Complementary?Jusri HadirmanNoch keine Bewertungen
- Welfare Services For Challenged ChildrenDokument42 SeitenWelfare Services For Challenged ChildrenRahul Dhaker70% (10)
- OT Practice October 8 IssueDokument21 SeitenOT Practice October 8 IssueThe American Occupational Therapy AssociationNoch keine Bewertungen
- 2019-09-01 Mens Health Singapore PDFDokument84 Seiten2019-09-01 Mens Health Singapore PDFaman singhNoch keine Bewertungen
- Scorebuilders 2Dokument40 SeitenScorebuilders 2Kilopop Man100% (1)
- So Important 4Dokument28 SeitenSo Important 4sundus youssefNoch keine Bewertungen
- Cognitive Rehabilitation: Model For Occupational Therapy: Beatriz Colon Abreu, Joan Pascale TogliaDokument10 SeitenCognitive Rehabilitation: Model For Occupational Therapy: Beatriz Colon Abreu, Joan Pascale Togliavandrade_635870Noch keine Bewertungen
- 3&epublic of Tbe Tlbtltpptnes Upre1ne '1:ourtDokument13 Seiten3&epublic of Tbe Tlbtltpptnes Upre1ne '1:ourtCesar ValeraNoch keine Bewertungen
- The Effects of Recreation Therapy On The Habit of Smoking and Positive-Negative Symptoms Among Patients With Chronic SchizophreniaDokument5 SeitenThe Effects of Recreation Therapy On The Habit of Smoking and Positive-Negative Symptoms Among Patients With Chronic SchizophreniaTeodorNoch keine Bewertungen
- NCP PcapDokument2 SeitenNCP PcapKenj Pereña100% (1)
- Request For Proposal (RFP) #4794 Physiotherapy Services: Sponsored by Health PEI - Community Hospitals WestDokument29 SeitenRequest For Proposal (RFP) #4794 Physiotherapy Services: Sponsored by Health PEI - Community Hospitals WestDiganta DasNoch keine Bewertungen
- COM 1013 Course Outline 2023-20241Dokument10 SeitenCOM 1013 Course Outline 2023-20241PauloNoch keine Bewertungen
- A CBT-based Approach To Medically Unexplained Symptoms: ArticleDokument7 SeitenA CBT-based Approach To Medically Unexplained Symptoms: Articleaastha jainNoch keine Bewertungen
- Emma Cohen Resume MsotDokument2 SeitenEmma Cohen Resume Msotapi-362293951Noch keine Bewertungen
- Military and War Contribution To OT and Hand TherapyDokument9 SeitenMilitary and War Contribution To OT and Hand TherapyKwende89Noch keine Bewertungen
- Applying A Holistic Hamstring Injury Prevention Approach in Elite Football: 12 Seasons, Single Club StudyDokument14 SeitenApplying A Holistic Hamstring Injury Prevention Approach in Elite Football: 12 Seasons, Single Club StudyjavierNoch keine Bewertungen
- Presidential Decree 1509, 1978Dokument5 SeitenPresidential Decree 1509, 1978VERA FilesNoch keine Bewertungen
- Amputation, Surgery and RehabilitationDokument46 SeitenAmputation, Surgery and RehabilitationPatrick WandellahNoch keine Bewertungen
- Code of Ethics V3Dokument2 SeitenCode of Ethics V3Rucsandra AvirvareiNoch keine Bewertungen