Das könnte Ihnen auch gefallen
- Multiple SclerosisDokument34 SeitenMultiple SclerosisDe Sesto Rhys Carlo0% (1)
- Multiple SclerosisDokument4 SeitenMultiple Sclerosisapi-3801039100% (1)
- Multiple SclerosisDokument8 SeitenMultiple SclerosisNader Smadi100% (1)
- Complications of Diabetes Mellitus-UpdateDokument48 SeitenComplications of Diabetes Mellitus-UpdateAnditha Namira RS100% (1)
- Myasthenia GravisDokument29 SeitenMyasthenia Gravisakash akash0% (1)
- AtherosclerosisDokument56 SeitenAtherosclerosisJohn Matley Caampued100% (8)
- Multiple SclerosisDokument68 SeitenMultiple Sclerosisvasant_goodoory100% (1)
- Raynaud's Disease - JERAIZADokument23 SeitenRaynaud's Disease - JERAIZAmaU439Noch keine Bewertungen
- Multiple SclerosisDokument2 SeitenMultiple Sclerosisplethoraldork100% (5)
- Cerebellar DisordersDokument51 SeitenCerebellar DisorderswasimNoch keine Bewertungen
- Peripheral NeuropathyDokument87 SeitenPeripheral NeuropathyAsaraf AliNoch keine Bewertungen
- Myasthenia Gravis BrochureDokument2 SeitenMyasthenia Gravis BrochureMolly100% (1)
- Cystic FibrosisDokument13 SeitenCystic Fibrosisgandhialpit100% (4)
- Myasthenia GravisDokument3 SeitenMyasthenia Gravisapi-3822433100% (2)
- Rheumatic Heart DiseaseDokument25 SeitenRheumatic Heart DiseaseMag5Noch keine Bewertungen
- Multiple Sclerosis: Case Study by Trcoski ElenaDokument43 SeitenMultiple Sclerosis: Case Study by Trcoski ElenaElena TrcoskiNoch keine Bewertungen
- CELLUTISDokument16 SeitenCELLUTISNorshahidah Ieda0% (1)
- Diabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40Dokument20 SeitenDiabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40HUSSAIN NAZEESHANoch keine Bewertungen
- Muscular DystrophyDokument33 SeitenMuscular DystrophyNurdina AfiniNoch keine Bewertungen
- Systemic Lupus Erythematosus (SLE) Is A Multiorgan System Autoimmune DiseaseDokument9 SeitenSystemic Lupus Erythematosus (SLE) Is A Multiorgan System Autoimmune Diseasecoyre100% (2)
- Tabes Dorsalis: Primary Stage: After The Initial InfectionDokument3 SeitenTabes Dorsalis: Primary Stage: After The Initial InfectionsekarananyaNoch keine Bewertungen
- Tuberculosis of KneeDokument17 SeitenTuberculosis of KneeJithin Bhagavati KalamNoch keine Bewertungen
- Rheumatoid ArthritisDokument9 SeitenRheumatoid ArthritisNader Smadi86% (7)
- LupusDokument28 SeitenLupusRiin IrasustaNoch keine Bewertungen
- OsteoarthritisDokument29 SeitenOsteoarthritischan park100% (1)
- Multiple SclerosisDokument44 SeitenMultiple SclerosisVijaya LakshmiNoch keine Bewertungen
- Multiple SclerosisDokument34 SeitenMultiple SclerosisRay YankeesNoch keine Bewertungen
- Multiple SclerosisDokument204 SeitenMultiple SclerosisOctavian Babcinschi100% (1)
- Current Trends in The Mangement of Cerebrovascular Accident: Lecture NotesDokument58 SeitenCurrent Trends in The Mangement of Cerebrovascular Accident: Lecture NotesBoas WayneNoch keine Bewertungen
- Multiple Sclerosis: Asif KianiDokument37 SeitenMultiple Sclerosis: Asif Kianiasifk124100% (2)
- CabgDokument12 SeitenCabgShreeja Sajit100% (1)
- Multiple SclerosisDokument3 SeitenMultiple SclerosisCarmella CollantesNoch keine Bewertungen
- Nephritic/nephrotic Syndrome.Dokument37 SeitenNephritic/nephrotic Syndrome.Kelechi OtamiriNoch keine Bewertungen
- Muscular DystrophyDokument3 SeitenMuscular Dystrophyderrickmason626Noch keine Bewertungen
- Parkinson's DiseaseDokument11 SeitenParkinson's Diseaseleeyan2wenty6100% (3)
- Multiple SclerosisDokument22 SeitenMultiple SclerosisJemai O. Bico ÜNoch keine Bewertungen
- Treatment and Management of Rheumatoid ArthritisDokument32 SeitenTreatment and Management of Rheumatoid ArthritisamirthaNoch keine Bewertungen
- Cerebellar InfarctionDokument23 SeitenCerebellar InfarctionShane LuyNoch keine Bewertungen
- Middle Cerebral ArteryDokument4 SeitenMiddle Cerebral Arterykat9210Noch keine Bewertungen
- Rheumatoid ArthritisDokument11 SeitenRheumatoid ArthritisCarmelita Christina100% (1)
- ANEURYSMDokument31 SeitenANEURYSMPooja Sahu100% (1)
- Parkinson DiseaseDokument14 SeitenParkinson DiseasemulfasatriaNoch keine Bewertungen
- Guillain Barre SyndromeDokument49 SeitenGuillain Barre SyndromeDavid SugiartoNoch keine Bewertungen
- Irritable Bowel SyndromeDokument13 SeitenIrritable Bowel SyndromeMay Ann ValledorNoch keine Bewertungen
- Motor Neuron DiseaseDokument23 SeitenMotor Neuron DiseasenicolasuttonNoch keine Bewertungen
- Hematological Alterations: Disseminated Intravascular Coagulation (DIC)Dokument16 SeitenHematological Alterations: Disseminated Intravascular Coagulation (DIC)jhommmmmNoch keine Bewertungen
- Spinal Cord InjuryDokument47 SeitenSpinal Cord InjuryShitaljit IromNoch keine Bewertungen
- Ewing's SarcomaDokument16 SeitenEwing's SarcomaChacha Zakiya100% (1)
- Nursing Management of Seizures and EpilepsyDokument36 SeitenNursing Management of Seizures and EpilepsyMatthew Ryan100% (6)
- Hodgkin's DiseaseDokument41 SeitenHodgkin's DiseaseDanilyn_Jumamo_1564100% (2)
- Rheumatoid ArthritisDokument13 SeitenRheumatoid ArthritisjhodaneNoch keine Bewertungen
- TuberculosisDokument4 SeitenTuberculosisdreamxtreme16100% (2)
- Presentation On Myasthenia Gravis: Presented By: Sandhya Harbola M.Sc. Nursing 1 Year PcnmsDokument32 SeitenPresentation On Myasthenia Gravis: Presented By: Sandhya Harbola M.Sc. Nursing 1 Year PcnmsShubham Singh Bisht100% (3)
- Reflex Sympathetic Dystrophy, CRPS-1Dokument47 SeitenReflex Sympathetic Dystrophy, CRPS-1Sayantika Dhar100% (1)
- Glasgow Coma Scale: - Eye-Opening - Motor - Verbal ResponsesDokument13 SeitenGlasgow Coma Scale: - Eye-Opening - Motor - Verbal ResponsesSofianNoch keine Bewertungen
- Rheumatic FeverDokument3 SeitenRheumatic FeverKhalid Mahmud Arifin100% (3)
- Multiple Sclerosis: Magaling, Julius Christian T. Roque, Patrick Vasallo, Rusella Paulina RDokument26 SeitenMultiple Sclerosis: Magaling, Julius Christian T. Roque, Patrick Vasallo, Rusella Paulina RSusie Rae FajardoNoch keine Bewertungen
- Multiple Sclerosis, Myasthenia Gravis, GBSDokument12 SeitenMultiple Sclerosis, Myasthenia Gravis, GBSpertinenteNoch keine Bewertungen
- U Y Y Y Y Y Ydisseminated SclerosisyyencephalomyelitisDokument5 SeitenU Y Y Y Y Y Ydisseminated Sclerosisyyencephalomyelitisnhie02Noch keine Bewertungen
- Multiple SclerosisDokument6 SeitenMultiple SclerosisMarife ManabatNoch keine Bewertungen
- Hirayama's DiseaseDokument27 SeitenHirayama's DiseaseDarshika Vyas MohanNoch keine Bewertungen
- Dandy Walker SyndromeDokument9 SeitenDandy Walker SyndromeDarshika Vyas MohanNoch keine Bewertungen
- Diffusion, Exchange & Transport of O2 & Co2Dokument79 SeitenDiffusion, Exchange & Transport of O2 & Co2Darshika Vyas MohanNoch keine Bewertungen
- Coma StimulationDokument18 SeitenComa StimulationDarshika Vyas Mohan88% (17)
- GuideDokument30 SeitenGuideBenjamin TantiansuNoch keine Bewertungen
- Multiple Sclerosis OfficialDokument20 SeitenMultiple Sclerosis OfficialJerin XavierNoch keine Bewertungen
- Demyelinating DiseasesDokument76 SeitenDemyelinating Diseasesapi-3743483100% (1)
- QB NeuroDokument30 SeitenQB Neurorichard bolinaoNoch keine Bewertungen
- Drug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver DiseaseDokument20 SeitenDrug-Induced Hepatotoxicity - Overview, Metabolism of Drugs, Clinical and Pathological Manifestations of Drug-Induced Liver Diseaseal ghiffari muhammad rayhan100% (1)
- Scleroza MultiplaDokument10 SeitenScleroza MultiplaTudor VoinaNoch keine Bewertungen
- Multiple SclerosisDokument21 SeitenMultiple SclerosisjobinbionicNoch keine Bewertungen
- Neurorehabilitation 1Dokument439 SeitenNeurorehabilitation 1Duncan D'AmicoNoch keine Bewertungen
- Stability Fridge Meds PDFDokument22 SeitenStability Fridge Meds PDFJenny Jeong100% (1)
- Beyer2016 PDFDokument40 SeitenBeyer2016 PDFBilal AbbasNoch keine Bewertungen
- Multiple SclerosisDokument22 SeitenMultiple SclerosisJemai O. Bico ÜNoch keine Bewertungen
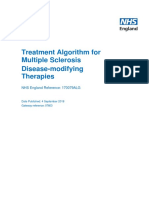
- Treatment Algorithm For Multiple Sclerosis Disease Modifying TherapiesDokument22 SeitenTreatment Algorithm For Multiple Sclerosis Disease Modifying TherapiesDiana StancaNoch keine Bewertungen
- Myasthenia Gravis, Alzheimers Disease, Multiple Sclerosis, Guillain-Barre Syndrome and Bell PalsyDokument9 SeitenMyasthenia Gravis, Alzheimers Disease, Multiple Sclerosis, Guillain-Barre Syndrome and Bell PalsyNielArmstrongNoch keine Bewertungen
- Multiple SclerosisDokument44 SeitenMultiple SclerosisVijaya LakshmiNoch keine Bewertungen
- Esclerosis Multiple y La Fatiga RelacionadaDokument20 SeitenEsclerosis Multiple y La Fatiga RelacionadaEdher PliegoNoch keine Bewertungen
- The Effects of A Yoga Intervention On Balance Speed and Endurance of Walking Fatigue and Quality of Life in People With Multiple SclerosisDokument8 SeitenThe Effects of A Yoga Intervention On Balance Speed and Endurance of Walking Fatigue and Quality of Life in People With Multiple SclerosisIsbah ShahidNoch keine Bewertungen
- Clinically Isolated Syndrome and Early Relapsing Multiple SclerosisDokument19 SeitenClinically Isolated Syndrome and Early Relapsing Multiple Sclerosisnight.shadowNoch keine Bewertungen
- Agnihotri Saurabh ResumeDokument6 SeitenAgnihotri Saurabh Resumesaurabh agnihotriNoch keine Bewertungen
- Treating Yourself Magazine #19Dokument132 SeitenTreating Yourself Magazine #19murciano207100% (4)
- Brain Atrophy in Multiple Sclerosis - Clinical Relevance and Technical Aspects (2017)Dokument12 SeitenBrain Atrophy in Multiple Sclerosis - Clinical Relevance and Technical Aspects (2017)Mahendri Deayu PutriNoch keine Bewertungen
- Cowen Therapeutic Outlook March 2009Dokument1.236 SeitenCowen Therapeutic Outlook March 2009Justin LachovskyNoch keine Bewertungen
- 2012 Biogen Idec Corporate Citizenship ReportDokument53 Seiten2012 Biogen Idec Corporate Citizenship ReportManpreet Singh SasanNoch keine Bewertungen
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDokument19 SeitenLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuNoch keine Bewertungen
- Multiple SclerosisDokument21 SeitenMultiple Sclerosisjhodane100% (1)
- List of Registered Drugs As of May 2012: DR No Generic Brand Strength Form CompanyDokument16 SeitenList of Registered Drugs As of May 2012: DR No Generic Brand Strength Form CompanybgtbingoNoch keine Bewertungen
- Analytical QuestionsDokument29 SeitenAnalytical Questionsfujoji92Noch keine Bewertungen
- Fingolimoid - 2014Dokument9 SeitenFingolimoid - 2014rodicasept1967Noch keine Bewertungen
- Drugs Med-SurgTest 3Dokument6 SeitenDrugs Med-SurgTest 3Sarah PlunkettNoch keine Bewertungen
- TG Therapeutics Inc. (TGTX) - Reiterating Expectations For A Challenging Commercial Launch For Ublituximab SellDokument11 SeitenTG Therapeutics Inc. (TGTX) - Reiterating Expectations For A Challenging Commercial Launch For Ublituximab SellSergey KNoch keine Bewertungen
- Multiple SclerosisDokument91 SeitenMultiple SclerosisAaron James GrayNoch keine Bewertungen