Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Dr. Adeel Ahmed Waheed: House Officer M-4Dokument84 SeitenDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNoch keine Bewertungen
- Case Presentation ParaplegiaDokument51 SeitenCase Presentation ParaplegiaHussain Azhar100% (2)
- Checklist of Quality Indicators For NABH Accreditation PreparationDokument11 SeitenChecklist of Quality Indicators For NABH Accreditation PreparationQUALITY SIDARTH HOSPITALSNoch keine Bewertungen
- Approach To Unconsious PTDokument62 SeitenApproach To Unconsious PTHussain AzharNoch keine Bewertungen
- Medical Intensive Care UnitDokument120 SeitenMedical Intensive Care Unithaaronminalang100% (6)
- CotrimoxazoleDokument3 SeitenCotrimoxazolecsy123Noch keine Bewertungen
- Guided Prep Pack - Neet Mds 2021-22Dokument13 SeitenGuided Prep Pack - Neet Mds 2021-22Annu SharmaNoch keine Bewertungen
- Anam FinalDokument82 SeitenAnam FinalHussain AzharNoch keine Bewertungen
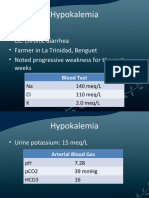
- HypokalemiaDokument12 SeitenHypokalemiaMohammad AliNoch keine Bewertungen
- K HomeosDokument47 SeitenK HomeosHussain AzharNoch keine Bewertungen
- Ion SyndromeDokument67 SeitenIon SyndromeHussain AzharNoch keine Bewertungen
- Liver Function Test FinalDokument98 SeitenLiver Function Test FinalHussain AzharNoch keine Bewertungen
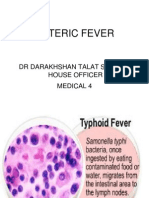
- Enteric FeverDokument63 SeitenEnteric FeverHussain AzharNoch keine Bewertungen
- Electrolyte Disturbaces - Hyponatremia and HypernatremiaDokument41 SeitenElectrolyte Disturbaces - Hyponatremia and HypernatremiaMohammad AliNoch keine Bewertungen
- Dka 31-05-11Dokument52 SeitenDka 31-05-11Hussain AzharNoch keine Bewertungen
- EFFA PRESENTATNhepatic EncephalopathyDokument50 SeitenEFFA PRESENTATNhepatic EncephalopathyHussain AzharNoch keine Bewertungen
- DVTDokument32 SeitenDVTHussain AzharNoch keine Bewertungen
- DKA Concepts and ManagementDokument22 SeitenDKA Concepts and ManagementMohammad AliNoch keine Bewertungen
- Dengue 2009Dokument53 SeitenDengue 2009Hussain AzharNoch keine Bewertungen
- DVT&PE Final 1Dokument59 SeitenDVT&PE Final 1Hussain AzharNoch keine Bewertungen
- CP Najma 97Dokument75 SeitenCP Najma 97Hussain AzharNoch keine Bewertungen
- Copd Final 97-2003hiraaDokument41 SeitenCopd Final 97-2003hiraaHussain AzharNoch keine Bewertungen
- AnemiaDokument37 SeitenAnemiaHussain AzharNoch keine Bewertungen
- Case Presentation 2Dokument53 SeitenCase Presentation 2Hussain AzharNoch keine Bewertungen
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDokument47 SeitenAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNoch keine Bewertungen
- Case Presentation Hypokalemic ManDokument61 SeitenCase Presentation Hypokalemic ManHussain AzharNoch keine Bewertungen
- AntibioticsDokument49 SeitenAntibioticsHussain AzharNoch keine Bewertungen
- Acute Renal FailureDokument120 SeitenAcute Renal FailureHussain AzharNoch keine Bewertungen
- An Approach To Anemic PatientDokument79 SeitenAn Approach To Anemic PatientHussain AzharNoch keine Bewertungen
- AKIDokument83 SeitenAKIHussain AzharNoch keine Bewertungen
- Acrf CDokument70 SeitenAcrf CHussain AzharNoch keine Bewertungen
- Acute Exacerbation of COPDDokument14 SeitenAcute Exacerbation of COPDMohammad AliNoch keine Bewertungen
- ABG S Final and Last TouchDokument88 SeitenABG S Final and Last TouchHussain AzharNoch keine Bewertungen
- Parkinson S Disease Epidemiology,.9Dokument5 SeitenParkinson S Disease Epidemiology,.9bacharelado2010Noch keine Bewertungen
- The Ivf Pack 2 PDFDokument11 SeitenThe Ivf Pack 2 PDFPaula BošnjakNoch keine Bewertungen
- Medoroga& Its ManagementDokument6 SeitenMedoroga& Its ManagementChintamani VeerrajuNoch keine Bewertungen
- Danish Mask StudyDokument1 SeiteDanish Mask StudyJuana AtkinsNoch keine Bewertungen
- Introduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologyDokument26 SeitenIntroduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologymochkurniawanNoch keine Bewertungen
- BSN 3-B (GROUP 2) - CLINICAL CASE ANALYSIS - Arthritis (REVISED)Dokument7 SeitenBSN 3-B (GROUP 2) - CLINICAL CASE ANALYSIS - Arthritis (REVISED)Florence Dumawal FariñasNoch keine Bewertungen
- Ultrasonic Surgical & Electrosurgical System: All in One Pla Orm, All With Superior PerformanceDokument2 SeitenUltrasonic Surgical & Electrosurgical System: All in One Pla Orm, All With Superior PerformanceDiego DulcamareNoch keine Bewertungen
- Eating Disorders Eating Disorders OverviewDokument12 SeitenEating Disorders Eating Disorders OverviewGiancarlo CrespoNoch keine Bewertungen
- Hypernatremia PediatricsDokument7 SeitenHypernatremia PediatricsJOHANNESKIFENDINoch keine Bewertungen
- Sensitivity and SpecificityDokument12 SeitenSensitivity and Specificitymia farrowNoch keine Bewertungen
- Frequency of Depression, Anxiety and Stress in Patients Referred For Endoscopy With Symptoms of DyspepsiaDokument5 SeitenFrequency of Depression, Anxiety and Stress in Patients Referred For Endoscopy With Symptoms of DyspepsiaSana SajidNoch keine Bewertungen
- CV Dr. Eko Arianto SpU 2021Dokument10 SeitenCV Dr. Eko Arianto SpU 2021Bedah ManadoNoch keine Bewertungen
- Chlorpromazine: Pharmacology Indications Contraindications Precautions Adverse Effects Overdose Dosage ResearchDokument36 SeitenChlorpromazine: Pharmacology Indications Contraindications Precautions Adverse Effects Overdose Dosage Researchnwaon4realNoch keine Bewertungen
- APAC Comarision of Registration Guidelines 2014 PDFDokument54 SeitenAPAC Comarision of Registration Guidelines 2014 PDFAnu PariyarathNoch keine Bewertungen
- Mrs. Manisha Chichani 29032023 064453 PMDokument1 SeiteMrs. Manisha Chichani 29032023 064453 PMManisha ChichaniNoch keine Bewertungen
- Sitecore - Media Library - Files.3d Imaging - Shared.7701 3dbrochure UsDokument28 SeitenSitecore - Media Library - Files.3d Imaging - Shared.7701 3dbrochure UsandiNoch keine Bewertungen
- 270 Scientists Call On Spotify To Take Action Over - Dangerous - Misinformation On Joe Rogan Podcast - IFLScienceDokument4 Seiten270 Scientists Call On Spotify To Take Action Over - Dangerous - Misinformation On Joe Rogan Podcast - IFLScienceDigiti inNoch keine Bewertungen
- Mental Health and Hindu Psicology by Swami AkhilanandaDokument245 SeitenMental Health and Hindu Psicology by Swami Akhilanandaapi-19985927100% (3)
- The Following Resources Related To This Article Are Available Online atDokument8 SeitenThe Following Resources Related To This Article Are Available Online atFerdina NidyasariNoch keine Bewertungen
- NCP EsrdDokument9 SeitenNCP EsrdMarisol Dizon100% (1)
- Maternal Care and ServicesDokument35 SeitenMaternal Care and ServicesAaron ConstantinoNoch keine Bewertungen
- Abnormal Illness BehaviorDokument7 SeitenAbnormal Illness Behavioransha2011p0% (1)
- Https Cghs - Nic.in Reports View Hospital - JSPDokument36 SeitenHttps Cghs - Nic.in Reports View Hospital - JSPRTI ActivistNoch keine Bewertungen
- Patent Ductus ArteriosusDokument31 SeitenPatent Ductus ArteriosussuderiNoch keine Bewertungen
- The Effect of Mangosteen (Garcinia Mangostana) Rind in The Blood Glucose Levels of Adult Patients With Type 2 Diabetes MellitusDokument4 SeitenThe Effect of Mangosteen (Garcinia Mangostana) Rind in The Blood Glucose Levels of Adult Patients With Type 2 Diabetes MellitusFiqoh Puteri FauziNoch keine Bewertungen
- Pre Op NCPDokument1 SeitePre Op NCPJoshua Kelly0% (2)