Das könnte Ihnen auch gefallen
- Shoulder DystociaDokument11 SeitenShoulder DystociaBrian CornelNoch keine Bewertungen
- I. Dystocia: A. CausesDokument9 SeitenI. Dystocia: A. CausesDianne GalangNoch keine Bewertungen
- 05 DystociaDokument10 Seiten05 DystociaRiantiara PutrizaNoch keine Bewertungen
- Shoulder DystociaDokument22 SeitenShoulder Dystociaamulan_aNoch keine Bewertungen
- Amniotic Fluid EmbolismDokument8 SeitenAmniotic Fluid EmbolismjNoch keine Bewertungen
- Dysfunctional Labor DystociaDokument8 SeitenDysfunctional Labor Dystociamardsz100% (2)
- Cesarean SectionDokument38 SeitenCesarean Sectionpat_rick_5Noch keine Bewertungen
- Instruments and Medications in Labour Room & OtDokument40 SeitenInstruments and Medications in Labour Room & OtIsaac TanNoch keine Bewertungen
- Pyloric StenosisDokument5 SeitenPyloric Stenosisensoooooooooo100% (1)
- HO 4 Essential Intrapartum Care 6may2013Dokument12 SeitenHO 4 Essential Intrapartum Care 6may2013Maedine Urbano-Briones100% (1)
- Uterine ProlapseDokument11 SeitenUterine ProlapseMelDred Cajes BolandoNoch keine Bewertungen
- CPD, Dystocia, Fetal Distress OutputDokument8 SeitenCPD, Dystocia, Fetal Distress OutputJohn Dave AbranNoch keine Bewertungen
- Φ PathophysiologyDokument4 SeitenΦ PathophysiologyMariah AshooriyanNoch keine Bewertungen
- Components of LaborDokument5 SeitenComponents of LaborJeraldine Lindo100% (4)
- CASE STUDY Labor and DeliveryDokument2 SeitenCASE STUDY Labor and DeliveryAprodite Sumod-ong100% (1)
- Live Preterm Baby Delivered NSDDokument13 SeitenLive Preterm Baby Delivered NSDKristine Anne SorianoNoch keine Bewertungen
- PolyhydramniosDokument2 SeitenPolyhydramniosAde Yonata100% (1)
- Assessment in PregnancyDokument15 SeitenAssessment in PregnancyAna75% (4)
- Cesarean SectionDokument61 SeitenCesarean SectionDaniel Ramos GomezNoch keine Bewertungen
- Case Stude NNJDokument6 SeitenCase Stude NNJmuzamirNoch keine Bewertungen
- CPDDokument45 SeitenCPDVijith.V.kumar100% (1)
- RH IncompatibilityDokument9 SeitenRH IncompatibilityJohn BardeenNoch keine Bewertungen
- Psychological Changes of PregnancyDokument30 SeitenPsychological Changes of PregnancyyuddNoch keine Bewertungen
- Retained PlacentaDokument2 SeitenRetained PlacentaAmiraah MasriNoch keine Bewertungen
- PartographDokument6 SeitenPartographYep Yep100% (2)
- What Is Retained PlacentaDokument7 SeitenWhat Is Retained PlacentaA Xiao Yhing TrancoNoch keine Bewertungen
- 68 Abnormal PeuperiumDokument44 Seiten68 Abnormal PeuperiumGodsonYeboah-AwudziNoch keine Bewertungen
- Pre Term LaborDokument3 SeitenPre Term LaborHazel Marie Echavez100% (1)
- Cord ProlapseDokument22 SeitenCord ProlapseJoyjet Evangelista-murilloNoch keine Bewertungen
- Incompetent CervixDokument5 SeitenIncompetent CervixNaidin Catherine De Guzman-Alcala100% (1)
- Ectopic Pregnancy - CSDokument14 SeitenEctopic Pregnancy - CSMASII100% (1)
- Pre and Post PregnancyDokument23 SeitenPre and Post PregnancyJitendra ChaudharyNoch keine Bewertungen
- Labor DystociaDokument100 SeitenLabor DystociaAnonymous kChMIy7tXNoch keine Bewertungen
- Shoulder PresentationDokument8 SeitenShoulder PresentationvincentsharonNoch keine Bewertungen
- Pregnancy Induced HypertensionDokument52 SeitenPregnancy Induced HypertensionJoy GloryNoch keine Bewertungen
- Case Study OligoDokument7 SeitenCase Study OligomutiaNoch keine Bewertungen
- Incomplete AbortionDokument18 SeitenIncomplete AbortionAra DirganNoch keine Bewertungen
- Wk1 - Introduction To Nursing ResearchDokument37 SeitenWk1 - Introduction To Nursing ResearchSophia GraziellaNoch keine Bewertungen
- Idiophatic Thrombocytopenic Purpura (ITP) in PregnancyDokument27 SeitenIdiophatic Thrombocytopenic Purpura (ITP) in PregnancyAdietya Bima PrakasaNoch keine Bewertungen
- High Risk PregnancyDokument6 SeitenHigh Risk PregnancyIyah Nicole100% (1)
- RH Incompatibility HandoutDokument4 SeitenRH Incompatibility HandoutMaricar Sanson FelicianoNoch keine Bewertungen
- Multiple PregnancyDokument20 SeitenMultiple PregnancySelma FraNoch keine Bewertungen
- Components of LaborDokument57 SeitenComponents of Laborangelus_eyes181996100% (1)
- Abnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Dokument34 SeitenAbnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Ana100% (3)
- Gestational Conditions 1Dokument19 SeitenGestational Conditions 1MrLarry Dolor100% (1)
- Shoulder Dystocia: Case AnalysisDokument16 SeitenShoulder Dystocia: Case AnalysisKurt Rovic Matza100% (1)
- Common Complications of PregnancyDokument34 SeitenCommon Complications of PregnancyiwennieNoch keine Bewertungen
- Topic # 2 PartographDokument42 SeitenTopic # 2 PartographJayrelle D. Safran100% (1)
- IUFDDokument2 SeitenIUFDnurseon0% (1)
- Spontaneous AbortionDokument8 SeitenSpontaneous Abortionsaber_fate_11Noch keine Bewertungen
- 3 (OB Cases)Dokument267 Seiten3 (OB Cases)Sharyl Plan SarominesNoch keine Bewertungen
- CASE STUDY: Pre Labor Infant With Respiratory Distress SyndromeDokument4 SeitenCASE STUDY: Pre Labor Infant With Respiratory Distress SyndromeE.R.ONoch keine Bewertungen
- Intrapartum Assessment: Factors That Affect Oxygenation During LaborDokument10 SeitenIntrapartum Assessment: Factors That Affect Oxygenation During LabornicewanNoch keine Bewertungen
- Postpartum Care - GLOWMDokument13 SeitenPostpartum Care - GLOWMAli KhaterNoch keine Bewertungen
- Leopold's Maneuver PDFDokument13 SeitenLeopold's Maneuver PDFBiway RegalaNoch keine Bewertungen
- Case Study For MaternalDokument2 SeitenCase Study For MaternalAcohCChaoNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Shoulder DystociaDokument2 SeitenShoulder DystociaManjiree KarandikarNoch keine Bewertungen
- Breech Delivery Shoulder Dystocia: James W. Van Hook, MDDokument21 SeitenBreech Delivery Shoulder Dystocia: James W. Van Hook, MDMansa SrivastavaNoch keine Bewertungen
- Breech PresentationDokument83 SeitenBreech PresentationJohn Ervin AgenaNoch keine Bewertungen
- Mother FatherDokument10 SeitenMother FatherAnonymousTargetNoch keine Bewertungen
- Emergency DeliveryDokument61 SeitenEmergency DeliveryRam Kirubakar ThangarajNoch keine Bewertungen
- Adolphe Pinard (1844-1934) of Paris and Intrauterine Paediatric CareDokument3 SeitenAdolphe Pinard (1844-1934) of Paris and Intrauterine Paediatric CareArliska WulandariNoch keine Bewertungen
- Labor ExerciseDokument2 SeitenLabor ExerciseDon RaulNoch keine Bewertungen
- InfertilityDokument224 SeitenInfertilityCota AncutaNoch keine Bewertungen
- Health Problems of Pregnant and Lactating WomanDokument45 SeitenHealth Problems of Pregnant and Lactating WomanSuraj Sahu100% (1)
- Care of The Mother and The Fetus During The Perinatal PeriodDokument22 SeitenCare of The Mother and The Fetus During The Perinatal PeriodRoshin Tejero100% (1)
- 092110101021-Silvi Eka Yuli KDokument5 Seiten092110101021-Silvi Eka Yuli Kmutiara syifaNoch keine Bewertungen
- Second Quarter Sps Test - Grade 5Dokument2 SeitenSecond Quarter Sps Test - Grade 5Mitchz TrinosNoch keine Bewertungen
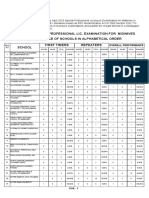
- April 2023 Special Professional Lic. Examination For MidwivesDokument2 SeitenApril 2023 Special Professional Lic. Examination For MidwivesRapplerNoch keine Bewertungen
- MCN ReviewerDokument2 SeitenMCN ReviewerJunghoon YangParkNoch keine Bewertungen
- Form 11Dokument1 SeiteForm 11Nurul Huda KhanNoch keine Bewertungen
- Anomalies of The Placenta and Cord 1Dokument52 SeitenAnomalies of The Placenta and Cord 1Daniel Andre S. Somoray100% (1)
- MoringaDokument29 SeitenMoringaDromic FO 11Noch keine Bewertungen
- Gonorrhea Fact SheetDokument2 SeitenGonorrhea Fact SheetRebecca Richardson0% (1)
- Juli 2022Dokument28 SeitenJuli 2022Chynthea ParamithaNoch keine Bewertungen
- Delivery Room FocusDokument4 SeitenDelivery Room FocusCarmela Dawn Marco100% (2)
- Baby Shower TabooDokument4 SeitenBaby Shower Taboosarahslist100% (9)
- In Vitro Fertilization - 2019-01-09Dokument5 SeitenIn Vitro Fertilization - 2019-01-09Priyanshu amanNoch keine Bewertungen
- Giving Birth: Learning Objectives: After The Discussion of This Topic, You Should Be Able ToDokument126 SeitenGiving Birth: Learning Objectives: After The Discussion of This Topic, You Should Be Able Tochesca_paunganNoch keine Bewertungen
- BEmONC - Training ManualDokument263 SeitenBEmONC - Training ManualdiribaNoch keine Bewertungen
- Post PartumDokument35 SeitenPost PartumLiza Marie Cayetano AdarneNoch keine Bewertungen
- 12 Friedmans Curve v2Dokument4 Seiten12 Friedmans Curve v2Jowi Sal100% (1)
- ObstetricDokument4 SeitenObstetricIsabel Bibat DavidNoch keine Bewertungen
- Feeding of Normal AND Low Birth Weight Babies: Amola Khandwala Under Guidance of DR Dipen PatelDokument54 SeitenFeeding of Normal AND Low Birth Weight Babies: Amola Khandwala Under Guidance of DR Dipen PatelDeep ShahNoch keine Bewertungen
- Miscarriage: - Nur Farhanah Binti Syed Abu Thahir - Hema Latha A/P Manickam - Fathin Fahrieza Binti Mohd AtanDokument33 SeitenMiscarriage: - Nur Farhanah Binti Syed Abu Thahir - Hema Latha A/P Manickam - Fathin Fahrieza Binti Mohd AtanIsmail FaruqiNoch keine Bewertungen
- MenopauseDokument4 SeitenMenopauseStella CooKeyNoch keine Bewertungen
- Medical Narrative Report On Child DeliveryDokument3 SeitenMedical Narrative Report On Child DeliveryMelona BenidoNoch keine Bewertungen
- CR Duty 09.05.2019Dokument87 SeitenCR Duty 09.05.2019R Ismail HadyathmaNoch keine Bewertungen