Das könnte Ihnen auch gefallen
- Public Health - Resume of Shah BookDokument54 SeitenPublic Health - Resume of Shah BookKami Dhillon83% (6)
- Augmented Intelligence The Next Frontier (English - White Paper)Dokument12 SeitenAugmented Intelligence The Next Frontier (English - White Paper)Nitesh LaguriNoch keine Bewertungen
- Clinical Audit On Diabetic Retinopathy ScreeningDokument1 SeiteClinical Audit On Diabetic Retinopathy ScreeningJeffrey Elvin100% (1)
- AGREE Reporting Checklist 2016Dokument4 SeitenAGREE Reporting Checklist 2016Jimmy ZhangNoch keine Bewertungen
- Decision On DiagnosisDokument13 SeitenDecision On DiagnosisSam Raven Andres100% (1)
- Screening: Department of Public Health Medical School, University of PécsDokument38 SeitenScreening: Department of Public Health Medical School, University of PécsESSA GHAZWANI100% (1)
- BCB 411 - Lec 5Dokument10 SeitenBCB 411 - Lec 5NaushinKhanNoch keine Bewertungen
- Artificial Intelligence For Blood AnalysisDokument14 SeitenArtificial Intelligence For Blood AnalysisKIPNGENO EMMANUELNoch keine Bewertungen
- Performance Measures Using Electronic Health Records Five Case StudiesDokument46 SeitenPerformance Measures Using Electronic Health Records Five Case StudieswmhoggNoch keine Bewertungen
- Price Analytics: Dr. Keerti Jain NIIT University, NeemranaDokument88 SeitenPrice Analytics: Dr. Keerti Jain NIIT University, NeemranaTushar GoelNoch keine Bewertungen
- F-05 814 Pricing StrategyDokument24 SeitenF-05 814 Pricing Strategydinosaur2512Noch keine Bewertungen
- Gen MatrixDokument36 SeitenGen MatrixPrakash VadavadagiNoch keine Bewertungen
- Base Slides - Pricing PDFDokument58 SeitenBase Slides - Pricing PDFvitrahulNoch keine Bewertungen
- Bio MarkersDokument19 SeitenBio MarkersassumptaNoch keine Bewertungen
- Remote Patient Monitoring System With Focused Research On Vital Signs Through Sensors BS (CS) 13 BatchDokument10 SeitenRemote Patient Monitoring System With Focused Research On Vital Signs Through Sensors BS (CS) 13 BatchBaSit ALi DharejoNoch keine Bewertungen
- Health Prediction Using Data Mining - Scope DocumentDokument4 SeitenHealth Prediction Using Data Mining - Scope DocumentHaris AhmedNoch keine Bewertungen
- Diagnostic Imaging Global Market-Forecast To 2022Dokument4 SeitenDiagnostic Imaging Global Market-Forecast To 2022VinayNoch keine Bewertungen
- Sales Territory Concept Designing & Functions and Qualities of Sales ExecutivesDokument22 SeitenSales Territory Concept Designing & Functions and Qualities of Sales ExecutivesStany D'melloNoch keine Bewertungen
- Health Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedDokument40 SeitenHealth Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedsmritiNoch keine Bewertungen
- Product Demo TemplateDokument9 SeitenProduct Demo Templateconnectadasgupta100% (1)
- Mls Imls Content Guideline PDFDokument11 SeitenMls Imls Content Guideline PDFswasahmedNoch keine Bewertungen
- NCD-Surveillance PPT Final 09132013 PDFDokument49 SeitenNCD-Surveillance PPT Final 09132013 PDFNur HusnulNoch keine Bewertungen
- Apex Institute of Engineering Department of Ait - Cse: B.E. CSE With Specialization in BDADokument13 SeitenApex Institute of Engineering Department of Ait - Cse: B.E. CSE With Specialization in BDARitika MakhariaNoch keine Bewertungen
- Gantt ChartDokument22 SeitenGantt ChartKanwal AliNoch keine Bewertungen
- System Health Monitoring and Prognostics - A ReviewDokument19 SeitenSystem Health Monitoring and Prognostics - A ReviewAamir AnisNoch keine Bewertungen
- Lec - 8 Steps of An OI (4-6)Dokument37 SeitenLec - 8 Steps of An OI (4-6)Hussein Omar Ali 212-41-1419Noch keine Bewertungen
- IT Infrastructure: Delivery MechanismDokument3 SeitenIT Infrastructure: Delivery MechanismJeyarajasekar TtrNoch keine Bewertungen
- Infographic IDP Vs OCR LatestDokument1 SeiteInfographic IDP Vs OCR LatestFund Exchange kidsNoch keine Bewertungen
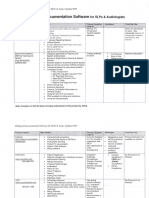
- Billing Documentation Software: For Slps AudiologistsDokument5 SeitenBilling Documentation Software: For Slps AudiologistsHoàng Đức NhuậnNoch keine Bewertungen
- Hospital EpidemiologymiologyDokument98 SeitenHospital EpidemiologymiologyRizky PebryanNoch keine Bewertungen
- HPEX 358-002 - Basics of EpidemiologyDokument31 SeitenHPEX 358-002 - Basics of EpidemiologyMichelle ValenzuelaNoch keine Bewertungen
- Research Analysis PDFDokument51 SeitenResearch Analysis PDFNoorain FirdouseNoch keine Bewertungen
- RT MDokument6 SeitenRT MShikhar NigamNoch keine Bewertungen
- Kotler Summary G-8Dokument3 SeitenKotler Summary G-8Varun KumarNoch keine Bewertungen
- Clinical Trial Course BrochureDokument11 SeitenClinical Trial Course BrochurechouguleNoch keine Bewertungen
- SPSSDokument92 SeitenSPSSBasílio HenriqueNoch keine Bewertungen
- Health Software Here 178Dokument23 SeitenHealth Software Here 178Morgan OkothNoch keine Bewertungen
- Cardiac BiomarkersDokument72 SeitenCardiac BiomarkersAmey JatharNoch keine Bewertungen
- Multivariate AnalysisDokument15 SeitenMultivariate Analysisshivakumar NNoch keine Bewertungen
- Lean & Six Sigma For Clinical Laboratory by DR Annabel DSouza SekarDokument27 SeitenLean & Six Sigma For Clinical Laboratory by DR Annabel DSouza Sekartaenia_proNoch keine Bewertungen
- Pai - Lecture4 - Measures of Effect and ImpactDokument54 SeitenPai - Lecture4 - Measures of Effect and ImpactAndry KurniadiNoch keine Bewertungen
- Applied Statistics II-2 and IIIDokument59 SeitenApplied Statistics II-2 and IIIMagnifico FangaWoroNoch keine Bewertungen
- Lecture Notes On Epidemiological Studies For UndergraduatesDokument41 SeitenLecture Notes On Epidemiological Studies For UndergraduatespopasorinemilianNoch keine Bewertungen
- Environmental EpidemiologyDokument5 SeitenEnvironmental EpidemiologyKarthik VkNoch keine Bewertungen
- Multivariate Analysis: Dr. Raghuvir SinghDokument13 SeitenMultivariate Analysis: Dr. Raghuvir SinghTush SinghalNoch keine Bewertungen
- 2012 BasicsOfSPSS Part2Dokument93 Seiten2012 BasicsOfSPSS Part2Tarm TawanNoch keine Bewertungen
- Delivering Cloud-Based Solutions For Hospitals, Physicians, Clinics, Patients, and PopulationDokument4 SeitenDelivering Cloud-Based Solutions For Hospitals, Physicians, Clinics, Patients, and PopulationsomyaNoch keine Bewertungen
- Embedded Based Real-Time Patient Monitoring SystemDokument5 SeitenEmbedded Based Real-Time Patient Monitoring SystemTabithaDsouza50% (2)
- Thyroid Scintigraphy-Coass RadiologiDokument29 SeitenThyroid Scintigraphy-Coass RadiologiBerlianaiiNoch keine Bewertungen
- Multiple Regression: Dr. Sanjay Rastogi IIFT, New DelhiDokument37 SeitenMultiple Regression: Dr. Sanjay Rastogi IIFT, New Delhisatishreddy71Noch keine Bewertungen
- 02 Measures of AssociationDokument67 Seiten02 Measures of AssociationAhmed HassanNoch keine Bewertungen
- Count Data Analysis Using Poisson Regression: University of Southeastern Philippines Advanced Studies Mintal, Davao CityDokument19 SeitenCount Data Analysis Using Poisson Regression: University of Southeastern Philippines Advanced Studies Mintal, Davao Citydanna ibanezNoch keine Bewertungen
- Kleinbaum-Klein2012 Chapter IntroductionToSurvivalAnalysisDokument54 SeitenKleinbaum-Klein2012 Chapter IntroductionToSurvivalAnalysisagNoch keine Bewertungen
- Infectious Diseases. Etiology PDFDokument76 SeitenInfectious Diseases. Etiology PDFIoana CozmaNoch keine Bewertungen
- Introduction To Biostatistics1Dokument23 SeitenIntroduction To Biostatistics1Noha SalehNoch keine Bewertungen
- GEHC White Papers Digital PathologyDokument13 SeitenGEHC White Papers Digital PathologySoodn Kang SoodnNoch keine Bewertungen
- Brain ScintigraphyDokument24 SeitenBrain ScintigraphyDustin Miranda100% (1)
- Multivariate AnaDokument20 SeitenMultivariate AnaNIKNISHNoch keine Bewertungen
- Interpret Market Trends and Developments TASk 1Dokument7 SeitenInterpret Market Trends and Developments TASk 1Raí SilveiraNoch keine Bewertungen
- l3 Measures of Population Impact and Infectiouness NotesDokument9 Seitenl3 Measures of Population Impact and Infectiouness Notestheus_35Noch keine Bewertungen
- Research Methods & Reporting: STARD 2015: An Updated List of Essential Items For Reporting Diagnostic Accuracy StudiesDokument9 SeitenResearch Methods & Reporting: STARD 2015: An Updated List of Essential Items For Reporting Diagnostic Accuracy StudiesJorge Villoslada Terrones100% (1)
- Remote Medical Monitoring A Complete Guide - 2021 EditionVon EverandRemote Medical Monitoring A Complete Guide - 2021 EditionNoch keine Bewertungen
- Epi & StatisticsDokument135 SeitenEpi & StatisticsFatma AlSayeghNoch keine Bewertungen
- Measurment of Health Edited PDFDokument347 SeitenMeasurment of Health Edited PDFBekele AberaNoch keine Bewertungen
- Drug-Free Workplace PolicyDokument5 SeitenDrug-Free Workplace PolicyRez BasilaNoch keine Bewertungen
- Global Cancer Facts and Figures 4th EditionDokument76 SeitenGlobal Cancer Facts and Figures 4th EditionAfra AmiraNoch keine Bewertungen
- Criteria For ScreeningDokument13 SeitenCriteria For Screeningabisoniya17Noch keine Bewertungen
- Assessing The Validity and Reliability of Diagnostic and Screening TestsDokument38 SeitenAssessing The Validity and Reliability of Diagnostic and Screening Testssarguss1467% (3)
- Screening and Pharmacy 2019 - TM02Dokument48 SeitenScreening and Pharmacy 2019 - TM02A'Ilda MNoch keine Bewertungen
- Fall 2023 Health Trends ReportDokument17 SeitenFall 2023 Health Trends ReportLaura LizarazoNoch keine Bewertungen
- The Biology of CancerDokument20 SeitenThe Biology of CancerAlishka Garg59% (22)
- Studi Kasus Teori Pemodelan SistemDokument14 SeitenStudi Kasus Teori Pemodelan SistemRenaldo Yoku100% (1)
- The Effectiveness of Triggering On Improving Motivation and Participation in A Cervical Cancer Screening Program in KediriDokument8 SeitenThe Effectiveness of Triggering On Improving Motivation and Participation in A Cervical Cancer Screening Program in KediriAmaliaNoch keine Bewertungen
- 2020 MLB Operations ManualDokument101 Seiten2020 MLB Operations ManualHouston Chronicle100% (5)
- Breast Self Examination Literature ReviewDokument8 SeitenBreast Self Examination Literature Reviewcjxfjjvkg100% (1)
- BreastDokument8 SeitenBreastOkea ClintonNoch keine Bewertungen
- Vitamin D ScreeningDokument7 SeitenVitamin D ScreeningMaryam FadahNoch keine Bewertungen
- Knowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Ethiopian Health Care WorkersDokument10 SeitenKnowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Ethiopian Health Care WorkersSrideviRaviNoch keine Bewertungen
- Ra 9288Dokument7 SeitenRa 9288bhebski1905Noch keine Bewertungen
- (CPG) Philippine Clinical Practice Guidelines For The Screening and Diagnosis of Obesity in AdultsDokument112 Seiten(CPG) Philippine Clinical Practice Guidelines For The Screening and Diagnosis of Obesity in AdultsMARIELLE GARCIANoch keine Bewertungen
- Review 4 ADokument67 SeitenReview 4 AAdish vianNoch keine Bewertungen
- Congenital Heart Disease Screening Modified Peds.2017-4065.FullDokument9 SeitenCongenital Heart Disease Screening Modified Peds.2017-4065.FullRene H. Framcisco, MDNoch keine Bewertungen
- Owens - Ba (2021) Economics of Policing & Public SaftyDokument26 SeitenOwens - Ba (2021) Economics of Policing & Public SaftywildcardNoch keine Bewertungen
- Roche Products and Diagno.Dokument132 SeitenRoche Products and Diagno.Mahmoud Ahmed100% (2)
- Paper 1: Concept of Health and DiseaseDokument7 SeitenPaper 1: Concept of Health and DiseaseYash LohiyaNoch keine Bewertungen
- Screening For Depression in GP From Patient-UkDokument2 SeitenScreening For Depression in GP From Patient-UkRosie AmerikanouNoch keine Bewertungen
- CC1 Lect - Overview of CC IndDokument2 SeitenCC1 Lect - Overview of CC IndJ Pao Bayro LacanilaoNoch keine Bewertungen
- Airport Preparedness Guidelines For Outbreaks of Communicable PDFDokument8 SeitenAirport Preparedness Guidelines For Outbreaks of Communicable PDFPrateek KishoreNoch keine Bewertungen
- Nontraumatic Osteonecrosis of The Femoral Head: Ten Years LaterDokument16 SeitenNontraumatic Osteonecrosis of The Femoral Head: Ten Years LaterChristian OliveiraNoch keine Bewertungen
- 1 40Dokument51 Seiten1 40bsmallahNoch keine Bewertungen