Das könnte Ihnen auch gefallen
- Amniotomy ProcedureDokument4 SeitenAmniotomy ProcedureBlessy MadhuriNoch keine Bewertungen
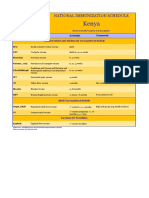
- Kenya Immunization ScheduleDokument1 SeiteKenya Immunization ScheduleDani AnyikaNoch keine Bewertungen
- Prepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Dokument53 SeitenPrepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Mir JavidNoch keine Bewertungen
- Chapter 43: Nursing Care of A Family When A Child Has An Infectious Disorder The Infectious Process #1 Infectious Disease in ChildrenDokument20 SeitenChapter 43: Nursing Care of A Family When A Child Has An Infectious Disorder The Infectious Process #1 Infectious Disease in ChildrenMark oliver Gonzales100% (1)
- Meningitis: Review ArticleDokument19 SeitenMeningitis: Review ArticleYo Me100% (1)
- Principles of Immunization: Vaccines, Definitions, and RecommendationsDokument18 SeitenPrinciples of Immunization: Vaccines, Definitions, and RecommendationsKibromWeldegiyorgisNoch keine Bewertungen
- Immunization LectureDokument32 SeitenImmunization LectureMekdes ZewdeNoch keine Bewertungen
- IMMUNIZATIO1 LatestDokument30 SeitenIMMUNIZATIO1 LatestAkshay H.Noch keine Bewertungen
- IMMUNIZATIONDokument35 SeitenIMMUNIZATIONAkshay H.Noch keine Bewertungen
- Immunization Review GPDokument46 SeitenImmunization Review GPKishore ChandkiNoch keine Bewertungen
- Immunitization and VaccinationDokument46 SeitenImmunitization and VaccinationMazhar RehmanNoch keine Bewertungen
- Standard Precaution LectureDokument12 SeitenStandard Precaution LecturearingkinkingNoch keine Bewertungen
- Infection Prevention and Control: DR Rahul KambleDokument61 SeitenInfection Prevention and Control: DR Rahul KambleDrRahul KambleNoch keine Bewertungen
- Infection and Prevention Control-2Dokument14 SeitenInfection and Prevention Control-2NIKHIL RAJNoch keine Bewertungen
- Japanese EncephalitisDokument10 SeitenJapanese Encephalitiskiki0% (1)
- Chapter 12 Basic ImmunologyDokument39 SeitenChapter 12 Basic ImmunologyTofikNoch keine Bewertungen
- Active and Passive ImmunizationDokument11 SeitenActive and Passive ImmunizationNgakanNoch keine Bewertungen
- (MMUNISATIONDokument54 Seiten(MMUNISATIONatharva sawantNoch keine Bewertungen
- The Differences Between Active and Passive ImmunizationDokument7 SeitenThe Differences Between Active and Passive ImmunizationRizwan AlamNoch keine Bewertungen
- Hemoglobin Estimation Methods GuideDokument23 SeitenHemoglobin Estimation Methods Guidekaran kambojNoch keine Bewertungen
- Epidemiology of Nosocomial Infections (Ncis) Part-1Dokument42 SeitenEpidemiology of Nosocomial Infections (Ncis) Part-1Indah IndrianiNoch keine Bewertungen
- Bordetella Pertussis and Whooping CoughDokument22 SeitenBordetella Pertussis and Whooping CoughDian TikaNoch keine Bewertungen
- AIIMS June 2020 - PSM QuestionsDokument7 SeitenAIIMS June 2020 - PSM QuestionsadiNoch keine Bewertungen
- Immunization QuizDokument4 SeitenImmunization QuizrrbischofbergerNoch keine Bewertungen
- Chickenpox: Suraj AhirwarDokument27 SeitenChickenpox: Suraj Ahirwardhanaraj4uNoch keine Bewertungen
- Recent Trends in Viral VaccinesDokument64 SeitenRecent Trends in Viral VaccinesAkula Sai PrasannaNoch keine Bewertungen
- M U M P S: Dr.T.V.Rao MDDokument35 SeitenM U M P S: Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- Gilut Herpes ZosteRDokument24 SeitenGilut Herpes ZosteRdimasahadiantoNoch keine Bewertungen
- PID: Understanding Pelvic Inflammatory DiseaseDokument34 SeitenPID: Understanding Pelvic Inflammatory Diseaseraed faisalNoch keine Bewertungen
- Pharmacodynamics of AntibioticsDokument28 SeitenPharmacodynamics of AntibioticsHazimMahmoudDarwishNoch keine Bewertungen
- Care BundlesDokument4 SeitenCare Bundlesmikhaela saboNoch keine Bewertungen
- SANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION BDokument15 SeitenSANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION Bsandra0% (1)
- HepB-Group5-AcuteChronicStagesTransmissionPreventionDokument17 SeitenHepB-Group5-AcuteChronicStagesTransmissionPreventiononijinoNoch keine Bewertungen
- RMNCAH Quality Improvement QI FrameworkDokument82 SeitenRMNCAH Quality Improvement QI FrameworkShahidul Islam ChowdhuryNoch keine Bewertungen
- Expanded Program On ImmunizationDokument7 SeitenExpanded Program On ImmunizationVanessa Abboud100% (1)
- Trichomoniasis: T. Vaginalis Is A Parasitic Protozoan, and The Taxonomic Position Is Based On The ClassificationDokument15 SeitenTrichomoniasis: T. Vaginalis Is A Parasitic Protozoan, and The Taxonomic Position Is Based On The Classificationrave robNoch keine Bewertungen
- Community Nutrition ProgrammesDokument44 SeitenCommunity Nutrition ProgrammesNeethu VincentNoch keine Bewertungen
- Bacterial VaccineDokument44 SeitenBacterial VaccineShrenik LuniyaNoch keine Bewertungen
- Definitions and Pillars For Safemother HoodDokument39 SeitenDefinitions and Pillars For Safemother HoodMayom Mabuong50% (4)
- LP 4-ImmunoprophylaxisDokument15 SeitenLP 4-ImmunoprophylaxismlinaballerinaNoch keine Bewertungen
- Source of Infections 1. Endogenous SourceDokument6 SeitenSource of Infections 1. Endogenous SourceDeepu VijayaBhanuNoch keine Bewertungen
- Universal Precaution by FithriDokument62 SeitenUniversal Precaution by FithriFithriKurniatiNoch keine Bewertungen
- Rabies FinalDokument18 SeitenRabies FinalPrem SinghNoch keine Bewertungen
- H.influenzae Modified 2012Dokument12 SeitenH.influenzae Modified 2012MoonAIRNoch keine Bewertungen
- Specimen Collection MicrobiologyDokument25 SeitenSpecimen Collection MicrobiologyHartiniNoch keine Bewertungen
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDokument28 SeitenElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- Chicken Pox PowerpointDokument9 SeitenChicken Pox PowerpointSean Schwartz0% (1)
- Vector-Borne Diseases in the Philippines: An OverviewDokument42 SeitenVector-Borne Diseases in the Philippines: An OverviewCyra Oynang100% (1)
- Vaccination (Immunization) : A Vaccine Is A Biological Preparation That Improves Immunity To A Particular DiseaseDokument21 SeitenVaccination (Immunization) : A Vaccine Is A Biological Preparation That Improves Immunity To A Particular Diseasemansi maheshwariNoch keine Bewertungen
- Tetanus: HistoryDokument15 SeitenTetanus: HistorydanielleNoch keine Bewertungen
- Blood Culture (Manual System)Dokument26 SeitenBlood Culture (Manual System)SAMMYNoch keine Bewertungen
- National Vector Borne Disease Control Programme StrategiesDokument53 SeitenNational Vector Borne Disease Control Programme StrategiesAditya NairNoch keine Bewertungen
- Reproductive Health 1Dokument18 SeitenReproductive Health 1hussain Altaher100% (1)
- Pertusis TreatmentDokument20 SeitenPertusis TreatmentJaipratap SinghNoch keine Bewertungen
- Universal Immunization ProgramDokument15 SeitenUniversal Immunization Programsmruti ranjanNoch keine Bewertungen
- Neonatal InfectionsDokument19 SeitenNeonatal InfectionsA B Siddique RiponNoch keine Bewertungen
- 1 Principles of First Aid and Its PracticeDokument118 Seiten1 Principles of First Aid and Its PracticeMohamed SamyNoch keine Bewertungen
- Autonomy of Nurse PDFDokument8 SeitenAutonomy of Nurse PDFDennis CobbNoch keine Bewertungen
- Malaria Parasites and Their Life CyclesDokument66 SeitenMalaria Parasites and Their Life CyclesDaxNoch keine Bewertungen
- 84 Vaccine Preventable Diseases and Immunization Programs FINAL 0 PDFDokument91 Seiten84 Vaccine Preventable Diseases and Immunization Programs FINAL 0 PDFhassanNoch keine Bewertungen
- Common Cold Symptoms, Treatment, and PreventionDokument3 SeitenCommon Cold Symptoms, Treatment, and Preventionanisa rimadhaniNoch keine Bewertungen
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesVon EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNoch keine Bewertungen
- Health 8 Q2 Mod 9 Get Immunized v2Dokument23 SeitenHealth 8 Q2 Mod 9 Get Immunized v2Ligaya BacuelNoch keine Bewertungen
- Q3-DLL HEALTH 8 - Wk1Dokument11 SeitenQ3-DLL HEALTH 8 - Wk1Krizelle Mae DublaNoch keine Bewertungen
- Community WrittenDokument23 SeitenCommunity WrittenImPrint CenterNoch keine Bewertungen
- MumpsDokument3 SeitenMumpsAbeer FatimaNoch keine Bewertungen
- A. Cotton Blue: False TrueDokument5 SeitenA. Cotton Blue: False TrueDevinViscars100% (1)
- Haemophilus Influenzae Type B Disease - 386,000 Deaths: Epidemics and OutbreaksDokument8 SeitenHaemophilus Influenzae Type B Disease - 386,000 Deaths: Epidemics and Outbreaksjames francis panganibanNoch keine Bewertungen
- Refusal of Recommended VaccinesDokument12 SeitenRefusal of Recommended VaccinesDr Dushyant Kamal Dhari100% (2)
- June 3, 2022 Summary Basis For Regulatory Action - PRIORIXDokument31 SeitenJune 3, 2022 Summary Basis For Regulatory Action - PRIORIXjaikp56Noch keine Bewertungen
- Importance of VaccinationDokument46 SeitenImportance of VaccinationTrixia Almiñe CervantesNoch keine Bewertungen
- Respiratory VirusesDokument123 SeitenRespiratory VirusesvaidyamNoch keine Bewertungen
- IM Assignment#4 Part5Section15Chapter202 MumpsDokument3 SeitenIM Assignment#4 Part5Section15Chapter202 MumpsJason OctavianoNoch keine Bewertungen
- QBANK PasTest Best of Fives For DentistryDokument165 SeitenQBANK PasTest Best of Fives For DentistrylindajenhaniNoch keine Bewertungen
- Slide 14 Diseases of Salivary Glands IDokument67 SeitenSlide 14 Diseases of Salivary Glands IJustDen09Noch keine Bewertungen
- MSM-Activate COM User's Guide v.4.4 (Micronetics) 1998Dokument32 SeitenMSM-Activate COM User's Guide v.4.4 (Micronetics) 1998TetuzinkriveisNoch keine Bewertungen
- NDA - BIO - CH 6 - DiseasesDokument4 SeitenNDA - BIO - CH 6 - Diseaseshemanth varsanNoch keine Bewertungen
- CampakDokument14 SeitenCampakNana YunusNoch keine Bewertungen
- Stefan Lanka The Misinterpretation of The Antibodies English TranslationDokument14 SeitenStefan Lanka The Misinterpretation of The Antibodies English Translationtrixstar108087Noch keine Bewertungen
- Detailed Lesson Plan in Mapeh 8Dokument13 SeitenDetailed Lesson Plan in Mapeh 8Jeoffrey ArceNoch keine Bewertungen
- Combine PDFDokument91 SeitenCombine PDFIbrahim SawaftaNoch keine Bewertungen
- Exam Quest Special 2023Dokument24 SeitenExam Quest Special 2023Yalvant YadavNoch keine Bewertungen
- MCN Oral RevalidaDokument11 SeitenMCN Oral RevalidaADOLF FRUELAN HIDALGONoch keine Bewertungen
- Meningitis ViralDokument7 SeitenMeningitis ViralTia Gustiani Poplei ViolaNoch keine Bewertungen
- Power PointDokument9 SeitenPower PointGabu BuNoch keine Bewertungen
- Pediatric Residency Training Authors and ContributorsDokument681 SeitenPediatric Residency Training Authors and ContributorsVictoria SandersNoch keine Bewertungen
- Autoimmunity Reviews: A. Greco, M. Fusconi, A. Gallo, C. Marinelli, G.F. Macri, M. de VincentiisDokument6 SeitenAutoimmunity Reviews: A. Greco, M. Fusconi, A. Gallo, C. Marinelli, G.F. Macri, M. de Vincentiisronaldyohanesf87Noch keine Bewertungen
- Community Medicine Solved KMU SEQs by RMC StudentsDokument106 SeitenCommunity Medicine Solved KMU SEQs by RMC StudentsAamir Khan67% (3)
- Virology Question Bank 2Dokument20 SeitenVirology Question Bank 2Jerin XavierNoch keine Bewertungen
- Communicable Disease Prevention GuideDokument197 SeitenCommunicable Disease Prevention Guidedennisjamesbartz100% (1)