Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
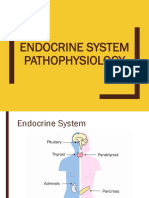
- Endocrine System (Pathophysiology)Dokument18 SeitenEndocrine System (Pathophysiology)roselle legson100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Insulin, Diabetes Oral HypoDokument94 SeitenInsulin, Diabetes Oral HypoNagu Kopparapu0% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Thyroid Disorder NCPDokument9 SeitenThyroid Disorder NCPKen RegalaNoch keine Bewertungen
- Pathology MnemonicsDokument27 SeitenPathology MnemonicsdyaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- UMS Medical Short Cases Records 1st EditionDokument36 SeitenUMS Medical Short Cases Records 1st EditionHendraDarmawan67% (3)
- Pathophysiology of HyperthyroidismDokument8 SeitenPathophysiology of Hyperthyroidismaasin100% (1)
- RECALLS DHA EXAM APRIL 2017 AnsweredDokument4 SeitenRECALLS DHA EXAM APRIL 2017 AnsweredDr-Jahanzaib Gondal100% (1)
- Immunosuppressant DrugsDokument87 SeitenImmunosuppressant DrugsNagu KopparapuNoch keine Bewertungen
- PuerperiumDokument85 SeitenPuerperiumHema MaliniNoch keine Bewertungen
- Diabetes MellitusDokument18 SeitenDiabetes Mellitusrajirajesh100% (1)
- vidya sagar reddy hospital kadapa - Google శోధన PDFDokument1 Seitevidya sagar reddy hospital kadapa - Google శోధన PDFNagu KopparapuNoch keine Bewertungen
- 44 Chloramphenicol, Tetracyclines, Macrolides, ClindamycinDokument77 Seiten44 Chloramphenicol, Tetracyclines, Macrolides, ClindamycinNagu KopparapuNoch keine Bewertungen
- Antifungals NagamaniDokument77 SeitenAntifungals NagamaniNagu KopparapuNoch keine Bewertungen
- The Fashion ChannelDokument4 SeitenThe Fashion ChannelmiranirfanNoch keine Bewertungen
- Thyroid Function TestingDokument12 SeitenThyroid Function TestingDewi Paramita YuniarahmiNoch keine Bewertungen
- Thyroid Gland Clinical Chemistry 2 (Laboratory) : LessonDokument4 SeitenThyroid Gland Clinical Chemistry 2 (Laboratory) : LessonCherry Ann ColechaNoch keine Bewertungen
- CARDIAC TUMORS Approach To ManagementDokument12 SeitenCARDIAC TUMORS Approach To ManagementAnkit GulatiNoch keine Bewertungen
- Thyroid Gland: Pactical Activity No. 5Dokument19 SeitenThyroid Gland: Pactical Activity No. 5Damian CorinaNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaJalalludin AnNoch keine Bewertungen
- Timolol Maleate Ophthalmic Solution, USP 0.25% and 0.5%: Comparative Product InformationDokument5 SeitenTimolol Maleate Ophthalmic Solution, USP 0.25% and 0.5%: Comparative Product InformationNur Utami PakayaNoch keine Bewertungen
- HypothyroidismDokument4 SeitenHypothyroidismDennis RosinNoch keine Bewertungen
- A Simplified Method For Diagnosis Ofgestational Age inDokument3 SeitenA Simplified Method For Diagnosis Ofgestational Age inLuis Salas GuzmanNoch keine Bewertungen
- Thyroid Testing Using RaiDokument8 SeitenThyroid Testing Using RaideblackaNoch keine Bewertungen
- The Thyroid ReviewDokument2 SeitenThe Thyroid Reviewwest alabamaNoch keine Bewertungen
- Levothyroxine SodiumDokument3 SeitenLevothyroxine Sodiumapi-3797941100% (1)
- Psychoimmunology Essay by DR Romesh Senewiratne-Alagaratnam (MD)Dokument32 SeitenPsychoimmunology Essay by DR Romesh Senewiratne-Alagaratnam (MD)Dr Romesh Arya Chakravarti100% (2)
- Management of Neonates Born To Mothers With Graves' Disease: BackgroundDokument13 SeitenManagement of Neonates Born To Mothers With Graves' Disease: BackgroundmariskaNoch keine Bewertungen
- Endocrine Physiology ReportDokument7 SeitenEndocrine Physiology ReportLeanne CubarNoch keine Bewertungen
- Endo MRCP NotesDokument41 SeitenEndo MRCP NotesVaanipriya RaoNoch keine Bewertungen
- 72 Endo AnnotatedDokument9 Seiten72 Endo AnnotatedErika ArceoNoch keine Bewertungen
- Antithyroid DrugsDokument52 SeitenAntithyroid DrugsYeyen MusainiNoch keine Bewertungen
- Diabetes Mellitus 1Dokument96 SeitenDiabetes Mellitus 1AkeroNoch keine Bewertungen
- Toxic AdenomaDokument5 SeitenToxic AdenomaRayan JabbarNoch keine Bewertungen
- Group2 Task A Medical Terms 1Dokument5 SeitenGroup2 Task A Medical Terms 1Jap MaligayoNoch keine Bewertungen
- Assessment & Management of Endocrine DisordersDokument45 SeitenAssessment & Management of Endocrine DisordersJerilee SoCute WattsNoch keine Bewertungen
- Surgery Sheet SchemeDokument51 SeitenSurgery Sheet SchemeReem E.MNoch keine Bewertungen