Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- CNM Test 1 FinalDokument264 SeitenCNM Test 1 FinalrayanNoch keine Bewertungen
- Ob Supplement Handout by DR - Chris SorianoDokument33 SeitenOb Supplement Handout by DR - Chris SorianoHedley Chua75% (4)
- Tantangan Kesehatan Mental Pada Periode Hamil, NifasDokument112 SeitenTantangan Kesehatan Mental Pada Periode Hamil, NifasAdefitriaNoch keine Bewertungen
- 11 Benefits of Breastfeeding For Both Mom and BabyDokument14 Seiten11 Benefits of Breastfeeding For Both Mom and BabyMac Cristian A. CaraganNoch keine Bewertungen
- The Impact of Teenage Pregnancy On Maternal, Fetal and Neonatal OutcomesDokument8 SeitenThe Impact of Teenage Pregnancy On Maternal, Fetal and Neonatal Outcomesjacque najeraNoch keine Bewertungen
- Uterine AtonyDokument3 SeitenUterine AtonyArsheina Paradji100% (1)
- MCN Menstrual Cycle LatestDokument8 SeitenMCN Menstrual Cycle LatestsophienNoch keine Bewertungen
- Inj. Ergometrine MaleatDokument17 SeitenInj. Ergometrine MaleatAarti RajputNoch keine Bewertungen
- Family Planning MethodDokument22 SeitenFamily Planning MethodPrince XianderNoch keine Bewertungen
- Menstrual Cycle An Ayurvedic ProspectiveDokument9 SeitenMenstrual Cycle An Ayurvedic ProspectiveRGuti13Noch keine Bewertungen
- Evaluation and Management of Primary Amenorrhea - UpToDateDokument14 SeitenEvaluation and Management of Primary Amenorrhea - UpToDateCristinaCaprosNoch keine Bewertungen
- Annotated Bibliography and SynthesisDokument6 SeitenAnnotated Bibliography and SynthesismperezveNoch keine Bewertungen
- Lactational Amenorrhea: Sumita Shakya Sushila Gautam Tila Sharma B.SC Nursing (2017)Dokument16 SeitenLactational Amenorrhea: Sumita Shakya Sushila Gautam Tila Sharma B.SC Nursing (2017)Sunita GurungNoch keine Bewertungen
- Antenatal Care Counseling: Roll No 11 To 23Dokument11 SeitenAntenatal Care Counseling: Roll No 11 To 23adityarathod612Noch keine Bewertungen
- Evaluation of The Endometrium For Malignant or Premalignant DiseaseDokument10 SeitenEvaluation of The Endometrium For Malignant or Premalignant Diseasenautilus81Noch keine Bewertungen
- A Journey To Safe Motherhood: Chiranjeevi Yojana GujaratDokument47 SeitenA Journey To Safe Motherhood: Chiranjeevi Yojana GujaratNeeraj SharmaNoch keine Bewertungen
- Soal Regarding Menoupause ConditionDokument6 SeitenSoal Regarding Menoupause ConditionfeliaNoch keine Bewertungen
- Carboprost TromethamineDokument2 SeitenCarboprost TromethamineDeathDefying DonutNoch keine Bewertungen
- InfertilityDokument10 SeitenInfertilityits_piks7256Noch keine Bewertungen
- Seminar On Obstructed LabourDokument98 SeitenSeminar On Obstructed Labourtesfahuntekletilahun80% (5)
- PGI MANIMTIM - Vaginal Delivery, Breech Delivery and Operative Vaginal DeliveryDokument8 SeitenPGI MANIMTIM - Vaginal Delivery, Breech Delivery and Operative Vaginal DeliveryKim Adarem Joy ManimtimNoch keine Bewertungen
- Anatomy and PhysiologyDokument8 SeitenAnatomy and Physiologyalynnavictoria67% (3)
- Conducting A Normal DeliveryDokument26 SeitenConducting A Normal DeliveryRedroses flowersNoch keine Bewertungen
- Mode of Delivery and Persistence of Pelvic Girdle Syndrome 6 Months PostpartumDokument20 SeitenMode of Delivery and Persistence of Pelvic Girdle Syndrome 6 Months PostpartumDanil ArmandNoch keine Bewertungen
- Topnotch Bridge Ob GyneDokument10 SeitenTopnotch Bridge Ob GyneAngela Saldajeno100% (1)
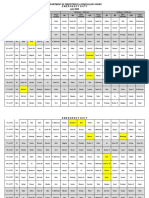
- Department of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020Dokument3 SeitenDepartment of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020noorNoch keine Bewertungen
- LESSON PLAN For COTDokument5 SeitenLESSON PLAN For COTMerrie Anne Pascual BagsicNoch keine Bewertungen
- Ovarian Cysts Overview: Menstrual Cycle Pregnancy UltrasoundDokument13 SeitenOvarian Cysts Overview: Menstrual Cycle Pregnancy Ultrasoundzerocoolz123Noch keine Bewertungen
- Recent Advancement in Infertility ManagementDokument18 SeitenRecent Advancement in Infertility ManagementFarheen khan100% (2)
- College of Medicine: Department of General SurgeryDokument53 SeitenCollege of Medicine: Department of General SurgeryAbdullah EssaNoch keine Bewertungen