Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
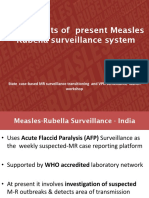
- 07a Ongoing MR Outbreak Surveillance SystemDokument23 Seiten07a Ongoing MR Outbreak Surveillance SystemDevendra Singh TomarNoch keine Bewertungen
- Pedia Revalida Exam: Email AddressDokument40 SeitenPedia Revalida Exam: Email AddressWilliam MilesNoch keine Bewertungen
- The Poultry Industry of Bangladesh An Overview CaseDokument6 SeitenThe Poultry Industry of Bangladesh An Overview CaseZarin Tanjim WoyshorjoNoch keine Bewertungen
- Use of Antibiotics in Periodontal TherapyDokument29 SeitenUse of Antibiotics in Periodontal TherapyBibek RajNoch keine Bewertungen
- Sputum AnalysisDokument12 SeitenSputum AnalysisAdriana GarciaNoch keine Bewertungen
- Icd 10Dokument1 SeiteIcd 10renatanurulNoch keine Bewertungen
- Ear DisorderDokument61 SeitenEar DisorderSakthi DeviNoch keine Bewertungen
- HealthCarePersonnelExposedToHCV AlgorithmDokument2 SeitenHealthCarePersonnelExposedToHCV Algorithmmmmaw mmNoch keine Bewertungen
- Hepa B Vaccine Consent FormDokument2 SeitenHepa B Vaccine Consent FormKESLEY DELOS SANTOSNoch keine Bewertungen
- TB/HIVDokument168 SeitenTB/HIVfikerteadelleNoch keine Bewertungen
- Textbook of Community Medicine PreventivDokument27 SeitenTextbook of Community Medicine Preventivtasneem faizaNoch keine Bewertungen
- Exam Preparation For BIOL1008: Infectious Diseases SectionDokument11 SeitenExam Preparation For BIOL1008: Infectious Diseases SectionEleanor LauNoch keine Bewertungen
- General Cleaning Disinfecting Guide: Canine LeptospirosisDokument2 SeitenGeneral Cleaning Disinfecting Guide: Canine LeptospirosisPATRICIA BROOKSNoch keine Bewertungen
- PyelonephritisDokument10 SeitenPyelonephritisalina abu rumi100% (1)
- Edid6508group 3 Storyboardcorrectedversion1Dokument35 SeitenEdid6508group 3 Storyboardcorrectedversion1api-349780383Noch keine Bewertungen
- Malaria NotesDokument3 SeitenMalaria NotesAbynarh PinaNoch keine Bewertungen
- Events 1 60 Recommended Articles of Events of Significance by AcetheCLATDokument392 SeitenEvents 1 60 Recommended Articles of Events of Significance by AcetheCLATTejash TapadiyaNoch keine Bewertungen
- Public HealthDokument19 SeitenPublic HealthOneofakind mnlNoch keine Bewertungen
- INFECTIONS Staphylococcal InfectionsDokument48 SeitenINFECTIONS Staphylococcal InfectionsDr.P.NatarajanNoch keine Bewertungen
- HerbologyDokument513 SeitenHerbologyVimal RajajiNoch keine Bewertungen
- Antibiotic Resistance and Persistence-Implications For Human Health and Treatment PerspectivesDokument24 SeitenAntibiotic Resistance and Persistence-Implications For Human Health and Treatment PerspectivesserviceNoch keine Bewertungen
- Alphabetical Listing of CLSI Books0309Dokument15 SeitenAlphabetical Listing of CLSI Books0309glodovichiNoch keine Bewertungen
- ChiroRab Press Release Nov 13 2019 PDFDokument2 SeitenChiroRab Press Release Nov 13 2019 PDFsr bNoch keine Bewertungen
- Review Indonesia Hayyat EnglishDokument14 SeitenReview Indonesia Hayyat EnglishhayyatNoch keine Bewertungen
- Chikungunya JENNIFERDokument29 SeitenChikungunya JENNIFERMarion Allen AlbaladejoNoch keine Bewertungen
- SVN 078 - 2021 - Migration Health Nurse II, Jakarta - 1Dokument4 SeitenSVN 078 - 2021 - Migration Health Nurse II, Jakarta - 1agnes febriyantiNoch keine Bewertungen
- A WGIHR2 6-EnDokument197 SeitenA WGIHR2 6-EnAzri 2906Noch keine Bewertungen
- Tuberculosis in Infancy and ChildhoodDokument32 SeitenTuberculosis in Infancy and ChildhoodArvin E. PamatianNoch keine Bewertungen
- Kode Icd 10Dokument29 SeitenKode Icd 10Zakia NisakNoch keine Bewertungen
- PEDIA Quiz 1Dokument3 SeitenPEDIA Quiz 1Cindy Mae MacamayNoch keine Bewertungen