Das könnte Ihnen auch gefallen
- Advanced Techniques For Repair and Rehabilitation in ConstructionDokument42 SeitenAdvanced Techniques For Repair and Rehabilitation in ConstructionNguyễn Hoàng Bảo50% (2)
- Past Simple and Present Perfect-OKDokument10 SeitenPast Simple and Present Perfect-OKnam_boc100% (1)
- Soil Investigation and Foundation DesignVon EverandSoil Investigation and Foundation DesignBewertung: 4.5 von 5 Sternen4.5/5 (9)
- Videos Export 2020 February 01 0008Dokument405 SeitenVideos Export 2020 February 01 0008eynon100% (2)
- Passport WalletDokument3 SeitenPassport WalletpotophanNoch keine Bewertungen
- Barbershop (TTBB A Cappella)Dokument7 SeitenBarbershop (TTBB A Cappella)Gustavo Espada100% (2)
- Baby Chick 2 in 1 Crochet PatternDokument7 SeitenBaby Chick 2 in 1 Crochet Patternchynthia.jmls100% (1)
- Hand Lay UpDokument29 SeitenHand Lay UpRavendran Krishnan100% (2)
- Module 2Dokument54 SeitenModule 2akash kumarNoch keine Bewertungen
- Types of Comedy in British-American LiteratureDokument5 SeitenTypes of Comedy in British-American LiteratureVanda Vigvári100% (1)
- Increasing the Durability of Paint and Varnish Coatings in Building Products and ConstructionVon EverandIncreasing the Durability of Paint and Varnish Coatings in Building Products and ConstructionNoch keine Bewertungen
- English For Travellers - BookletDokument98 SeitenEnglish For Travellers - BookletLorenita AraujoNoch keine Bewertungen
- Fly Love - From 2011 Animated Film RioDokument36 SeitenFly Love - From 2011 Animated Film RioCrispín Del Ángel HernándezNoch keine Bewertungen
- Pavement Design and ConstructionDokument82 SeitenPavement Design and Constructiondist2235Noch keine Bewertungen
- Technical Checklist: R.C.C. WorkDokument13 SeitenTechnical Checklist: R.C.C. WorkSiddharth GhorpadeNoch keine Bewertungen
- Sims 3 Serial KeyDokument4 SeitenSims 3 Serial KeyLabs Mendoza17% (6)
- Methods of Concrete Repair - 20181227 - KAYDokument24 SeitenMethods of Concrete Repair - 20181227 - KAYAmjadKhudaiNoch keine Bewertungen
- F - Fundamental Introduction To Pipeline Coatings - 2019Dokument119 SeitenF - Fundamental Introduction To Pipeline Coatings - 2019Shakeel AhmedNoch keine Bewertungen
- Unit IV Coating of Technical Textiles Coating TechniquesDokument55 SeitenUnit IV Coating of Technical Textiles Coating TechniquesPandurang Pawar100% (1)
- Protecting Steel Edges: Presented By: Bob Kogler, Rampart LLCDokument42 SeitenProtecting Steel Edges: Presented By: Bob Kogler, Rampart LLCSuperCow FelizNoch keine Bewertungen
- Assignment 2: Submitted To-Dr. Raju Sharma Submitted by - Arpan Singh Roll No - 801924004Dokument27 SeitenAssignment 2: Submitted To-Dr. Raju Sharma Submitted by - Arpan Singh Roll No - 801924004Arpan SidhuNoch keine Bewertungen
- Injection and Sealing of CracksDokument21 SeitenInjection and Sealing of CracksRagheb IbrahimNoch keine Bewertungen
- Block Adhesive Trowel and Application MethodDokument8 SeitenBlock Adhesive Trowel and Application MethodMoidin AfsanNoch keine Bewertungen
- Placing Technic Khun VICDokument22 SeitenPlacing Technic Khun VICSiamak HashempourNoch keine Bewertungen
- Manufacturing Process of Plywood: Presented By:-Group 2Dokument24 SeitenManufacturing Process of Plywood: Presented By:-Group 2rickNoch keine Bewertungen
- Investigation of Methods of Improving The Application Workmanship of WaterproofingDokument16 SeitenInvestigation of Methods of Improving The Application Workmanship of Waterproofingniran_udayangaNoch keine Bewertungen
- RefDokument33 SeitenRefMohamed KhaledNoch keine Bewertungen
- RefDokument33 SeitenRefMohamed KhaledNoch keine Bewertungen
- Design and Fabrication of Automatic Wall Plastering Machine PrototypeDokument6 SeitenDesign and Fabrication of Automatic Wall Plastering Machine Prototypeendalkachew gudetaNoch keine Bewertungen
- Internship PresentationDokument26 SeitenInternship PresentationHavanah AshuNoch keine Bewertungen
- B - Introduction To Coating - 2023 - Period 6Dokument61 SeitenB - Introduction To Coating - 2023 - Period 6aseNoch keine Bewertungen
- Methodology For ConcretingDokument4 SeitenMethodology For ConcretingVector DesignsNoch keine Bewertungen
- Himani Bansal Jayant Negi Ritesh Kumar Uday PratapDokument7 SeitenHimani Bansal Jayant Negi Ritesh Kumar Uday PratapJayant NegiNoch keine Bewertungen
- Hardened ConcreteDokument20 SeitenHardened Concretefaimy josephNoch keine Bewertungen
- Relining and RebasingDokument36 SeitenRelining and Rebasingفواز نميرNoch keine Bewertungen
- 2 ITATech Sprayed Membranes CelestinoDokument60 Seiten2 ITATech Sprayed Membranes CelestinoMarcelo ApoloNoch keine Bewertungen
- Reeta Summer InternshipDokument19 SeitenReeta Summer InternshipKapil Tu hi tuNoch keine Bewertungen
- Arba Minch Institution of Technology: Internshipreport ON Eprdf Traning CenterDokument23 SeitenArba Minch Institution of Technology: Internshipreport ON Eprdf Traning Centersamuel lireNoch keine Bewertungen
- EpoxyDokument19 SeitenEpoxyrexdindigulNoch keine Bewertungen
- Laboratory Activities 4, 5 and 6Dokument10 SeitenLaboratory Activities 4, 5 and 6REX IAN BONGALESNoch keine Bewertungen
- Microsoft Powerpoint - Tooth Colored Inlays and Onlays - IDokument53 SeitenMicrosoft Powerpoint - Tooth Colored Inlays and Onlays - Ianastoma100% (1)
- Pembaikan Bagi Kerosakan Bukan StrukturDokument26 SeitenPembaikan Bagi Kerosakan Bukan StrukturAnuar PadeliNoch keine Bewertungen
- Construction Method For Precast SystemDokument10 SeitenConstruction Method For Precast SystemKenny LiuNoch keine Bewertungen
- CT SMB Module 3Dokument31 SeitenCT SMB Module 3sankarsanasahoo690Noch keine Bewertungen
- Activity 10Dokument6 SeitenActivity 10srih89437Noch keine Bewertungen
- Lower Limb MCQsDokument65 SeitenLower Limb MCQsabq90Noch keine Bewertungen
- Government Engineering College Civil Engineering Department: Internship Project 2021-22Dokument23 SeitenGovernment Engineering College Civil Engineering Department: Internship Project 2021-22PranavRajsinh ZalaNoch keine Bewertungen
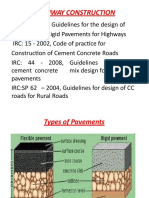
- Highway ConstructionDokument82 SeitenHighway ConstructionNavik BhandariNoch keine Bewertungen
- Experiment No. 01: S.A-I Laboratory Manual 1 Prepared By: Nishant SharmaDokument13 SeitenExperiment No. 01: S.A-I Laboratory Manual 1 Prepared By: Nishant Sharmasaket01nemaNoch keine Bewertungen
- Intermaxillary Relations RecordsDokument17 SeitenIntermaxillary Relations RecordsMega ShyamNoch keine Bewertungen
- 1.1 Overview of Public Work DepartmentDokument30 Seiten1.1 Overview of Public Work DepartmentSimran SinghNoch keine Bewertungen
- Frpmanufacturingmethods 151030103025 Lva1 App6891Dokument47 SeitenFrpmanufacturingmethods 151030103025 Lva1 App6891ABeer AkNoch keine Bewertungen
- Prostho MDC 22Dokument18 SeitenProstho MDC 22drberyl paulNoch keine Bewertungen
- Work Method Statement For IPS and Tremix FlooringDokument3 SeitenWork Method Statement For IPS and Tremix Flooringjohn paulNoch keine Bewertungen
- Gi - 4Dokument7 SeitenGi - 4Nehja ShajahanNoch keine Bewertungen
- Compaction 1Dokument15 SeitenCompaction 1Gopal SudhirNoch keine Bewertungen
- Muravyl Installation ENGDokument10 SeitenMuravyl Installation ENGjean paul florez herediaNoch keine Bewertungen
- F - Intro To Pipeline Coatings - 2023 - P7Dokument113 SeitenF - Intro To Pipeline Coatings - 2023 - P7aseNoch keine Bewertungen
- Concrete MixDokument24 SeitenConcrete MixAliñabo RoqueNoch keine Bewertungen
- Fire Proofing - ChartekDokument37 SeitenFire Proofing - ChartekOsama KheadryNoch keine Bewertungen
- Shallow FoundationDokument8 SeitenShallow FoundationSHELAR GAURINoch keine Bewertungen
- ReportDokument13 SeitenReportBroNoch keine Bewertungen
- Construction - 233Dokument56 SeitenConstruction - 233Shopmore PhilippinesNoch keine Bewertungen
- Construction - 23Dokument54 SeitenConstruction - 23Shopmore PhilippinesNoch keine Bewertungen
- K.pratyusha Assst - Prof, NECDokument9 SeitenK.pratyusha Assst - Prof, NECSaddaqatNoch keine Bewertungen
- Repair of Underwater Concrete StructuresDokument5 SeitenRepair of Underwater Concrete StructuresRaja babuNoch keine Bewertungen
- Experimental Study of Precast Portal Frame: 2Cl404 - Civil Engineering ProjectDokument93 SeitenExperimental Study of Precast Portal Frame: 2Cl404 - Civil Engineering Projectraja vijjayNoch keine Bewertungen
- Pressure Application MethodsDokument9 SeitenPressure Application Methodssyahmi sharifNoch keine Bewertungen
- Parc EstaDokument33 SeitenParc EstaAnonymous FcZX2N37XNoch keine Bewertungen
- Board Game LIVE: PE EditionDokument26 SeitenBoard Game LIVE: PE EditionNABELA YAHYANoch keine Bewertungen
- Improv 4Dokument2 SeitenImprov 4Mark Joseph Felicitas CuntapayNoch keine Bewertungen
- Asian Paint WF Stencil BookletDokument64 SeitenAsian Paint WF Stencil BookletspikysanchitNoch keine Bewertungen
- Datasheet - Vstream-For-Service-AssuranceDokument2 SeitenDatasheet - Vstream-For-Service-AssuranceKelvin PattyNoch keine Bewertungen
- TitanicDokument6 SeitenTitanicTeem ChakphetNoch keine Bewertungen
- Dance Terms Common To Philippine Folk DancesDokument7 SeitenDance Terms Common To Philippine Folk DancesSaeym SegoviaNoch keine Bewertungen
- The Singing SilenceDokument5 SeitenThe Singing Silencetishalikhar7Noch keine Bewertungen
- Our MenuDokument8 SeitenOur MenueatlocalmenusNoch keine Bewertungen
- DX DiagDokument47 SeitenDX Diagpg_rajuNoch keine Bewertungen
- S5 U1-2 MiniTestDokument3 SeitenS5 U1-2 MiniTestĐinh Thị Thu HàNoch keine Bewertungen
- 2170908Dokument19 Seiten2170908bhavikNoch keine Bewertungen
- PROFICIENCY 1 UNIT 4 (Sweet Rituals)Dokument61 SeitenPROFICIENCY 1 UNIT 4 (Sweet Rituals)Pablo GomesNoch keine Bewertungen
- Basic Fantasy Character Sheet Magic-User Rev.3Dokument2 SeitenBasic Fantasy Character Sheet Magic-User Rev.3vic neitteNoch keine Bewertungen
- David Child Biography and CritiquesDokument2 SeitenDavid Child Biography and CritiquesDavid Gómez HernándezNoch keine Bewertungen
- Lion Brand Lion Bouclé Beginner's One-Button JacketDokument4 SeitenLion Brand Lion Bouclé Beginner's One-Button Jacketmonica_lufoNoch keine Bewertungen
- JacintoCJNicole Laboratoryexercise1Dokument13 SeitenJacintoCJNicole Laboratoryexercise1Cj Nicole JacintoNoch keine Bewertungen
- Food - Countable and Uncountable NounsDokument5 SeitenFood - Countable and Uncountable NounsKenny GBNoch keine Bewertungen
- Marketing Cloud Data ViewsDokument1 SeiteMarketing Cloud Data Viewsajit jogiNoch keine Bewertungen
- Bridal Business PlanDokument16 SeitenBridal Business PlanFiker Er MarkNoch keine Bewertungen