Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
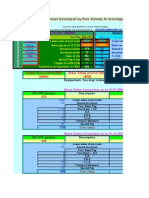
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Permissive AuthoriatDokument2 SeitenPermissive AuthoriatReiki KiranNoch keine Bewertungen
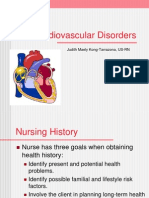
- Peripheral Vascular Diseases KDokument230 SeitenPeripheral Vascular Diseases Kjosephabram051590100% (4)
- Final Period - Assignment NCM 105Dokument3 SeitenFinal Period - Assignment NCM 105Chester NicoleNoch keine Bewertungen
- Parts and Functions of Respiratory SystemDokument18 SeitenParts and Functions of Respiratory Systemjosephabram051590Noch keine Bewertungen
- Recurrent Pregnancy LossDokument40 SeitenRecurrent Pregnancy LossJagannath MaaleNoch keine Bewertungen
- Burns and Wound Healing PDFDokument6 SeitenBurns and Wound Healing PDFJorge De VeraNoch keine Bewertungen
- 3 Intraoperative PhaseDokument28 Seiten3 Intraoperative Phaseada_beer100% (2)
- CASE STUDY Cesarean DeliveryDokument15 SeitenCASE STUDY Cesarean Deliverydirkdarren100% (3)
- How To Prepare For ADC 1Dokument2 SeitenHow To Prepare For ADC 1vermaz2deep100% (1)
- Pediatric AssessmentDokument62 SeitenPediatric AssessmentMaysa Ismail100% (4)
- Thermal BurnsDokument50 SeitenThermal BurnsPooya WindyNoch keine Bewertungen
- Cardiovascular ReviewDokument294 SeitenCardiovascular Reviewjosephabram051590Noch keine Bewertungen
- Nursing Practice StandardsDokument34 SeitenNursing Practice StandardsOmar Khalif Amad Pendatun100% (1)
- Implant FailureDokument6 SeitenImplant FailureNajeeb UllahNoch keine Bewertungen
- Novena Prayer To Our Lady of VailankanniDokument1 SeiteNovena Prayer To Our Lady of Vailankannijosephabram051590100% (1)
- Unang YakapDokument66 SeitenUnang YakapJeyneh Serafin100% (2)
- Antidotes To Commn MedicationDokument1 SeiteAntidotes To Commn Medicationjosephabram051590Noch keine Bewertungen
- Leadership Management Research Philnursingstudent ComDokument12 SeitenLeadership Management Research Philnursingstudent Comjosephabram051590Noch keine Bewertungen
- Hiv and AidsDokument40 SeitenHiv and Aidsjosephabram051590Noch keine Bewertungen
- Fundamentals Post Test Phil Nursing Student ComDokument13 SeitenFundamentals Post Test Phil Nursing Student Comjosephabram051590Noch keine Bewertungen
- A Teamwork Approach: To Quality Patient Care in The Operating RoomDokument14 SeitenA Teamwork Approach: To Quality Patient Care in The Operating Roomjosephabram051590Noch keine Bewertungen
- Nurse Practitioner and Clinical Nurse Specialist Competencies For Older Adult CareDokument36 SeitenNurse Practitioner and Clinical Nurse Specialist Competencies For Older Adult Carejosephabram051590Noch keine Bewertungen
- Nursing Care of Cancer Patients in Hospital and Home: 1958 8 122-129 Renilda HilkemeyerDokument7 SeitenNursing Care of Cancer Patients in Hospital and Home: 1958 8 122-129 Renilda Hilkemeyerjosephabram051590Noch keine Bewertungen
- Overview of Ethical PrinciplesDokument8 SeitenOverview of Ethical Principlesjosephabram051590Noch keine Bewertungen
- Neurological Problems and ManagementDokument52 SeitenNeurological Problems and Managementjosephabram051590Noch keine Bewertungen
- 70 Ways To Increase Your Brain PowerDokument8 Seiten70 Ways To Increase Your Brain PowertalktoankNoch keine Bewertungen
- Medical Precautions and Management of Illnesses and DiseasesDokument231 SeitenMedical Precautions and Management of Illnesses and Diseasesjosephabram051590Noch keine Bewertungen
- Orthopedic Problem and ManagementDokument42 SeitenOrthopedic Problem and Managementjosephabram051590Noch keine Bewertungen
- Syllabus FR Students Medsurg PCIDokument37 SeitenSyllabus FR Students Medsurg PCIjosephabram051590Noch keine Bewertungen
- Review Notes in Infection Control - NCLEXDokument1 SeiteReview Notes in Infection Control - NCLEXwyndz100% (10)
- MS ReviewDokument115 SeitenMS ReviewGrace Borja-MoralesNoch keine Bewertungen
- Nursing JurisprudenceDokument5 SeitenNursing Jurisprudencerifeman200791% (11)
- IV Essentials20071204Dokument23 SeitenIV Essentials20071204angie10231Noch keine Bewertungen
- Clinical Clerkship OncologyDokument136 SeitenClinical Clerkship Oncologyjosephabram051590100% (1)
- Fluid Electrolytes Acid-Base and ShockDokument18 SeitenFluid Electrolytes Acid-Base and Shockjosephabram051590100% (1)
- Newborn ScreeningDokument40 SeitenNewborn Screeningjosephabram051590Noch keine Bewertungen
- Acs Nstemi PathwayDokument3 SeitenAcs Nstemi PathwayAliey's SKeplek NgeNersNoch keine Bewertungen
- Benign Skin TumoursDokument7 SeitenBenign Skin TumoursMan LorNoch keine Bewertungen
- Resume Eportfolio Kerri HamiltonDokument2 SeitenResume Eportfolio Kerri Hamiltonapi-246968067Noch keine Bewertungen
- Unit 2 Chapter 8 Text For Diff Purposes - Doc 1Dokument11 SeitenUnit 2 Chapter 8 Text For Diff Purposes - Doc 1Seandrae PaeldenNoch keine Bewertungen
- Xarelto (Rivaroxaban) Toolkitfeb2015 PDFDokument11 SeitenXarelto (Rivaroxaban) Toolkitfeb2015 PDFSherly CanceritaNoch keine Bewertungen
- Fact Sheet Optic Nerve AtrophyDokument4 SeitenFact Sheet Optic Nerve Atrophyaryans1976Noch keine Bewertungen
- TumorDokument8 SeitenTumorputyCeria86Noch keine Bewertungen
- MastitisDokument13 SeitenMastitisapi-232713902Noch keine Bewertungen
- ReseachDokument3 SeitenReseachWen TingNoch keine Bewertungen
- Interview PaperDokument7 SeitenInterview Paperapi-253699105Noch keine Bewertungen
- Postoperative Care: Postoperative Note and OrdersDokument4 SeitenPostoperative Care: Postoperative Note and OrdersAhmedNoch keine Bewertungen
- 2 Marks Q & ADokument11 Seiten2 Marks Q & AJayaprakash JayaramanNoch keine Bewertungen
- Indian Ethos and Values in ManagementDokument23 SeitenIndian Ethos and Values in ManagementDinesh Babu PugalenthiNoch keine Bewertungen
- Lewis COPD Case StudyDokument2 SeitenLewis COPD Case Studyatarisgurl08Noch keine Bewertungen
- Naim Oral CareDokument34 SeitenNaim Oral Carenaim157Noch keine Bewertungen
- Local Anaesthesia PedoDokument28 SeitenLocal Anaesthesia PedoFourthMolar.com100% (1)
- Ubat Bah Ini :)Dokument172 SeitenUbat Bah Ini :)Eckry SilverNoch keine Bewertungen
- Decompressive Hemicraniectomy and DuroplastyDokument5 SeitenDecompressive Hemicraniectomy and DuroplastyAmy NilifdaNoch keine Bewertungen
- RRL For PrecisDokument4 SeitenRRL For PrecisDea SantellaNoch keine Bewertungen
- Nursing PhilosophyDokument6 SeitenNursing Philosophyapi-480550791Noch keine Bewertungen
- Community Health NursingDokument10 SeitenCommunity Health NursingBunzay GelineNoch keine Bewertungen