Beruflich Dokumente
Kultur Dokumente
10 1007@pl00001930
Hochgeladen von
selvam123456789Originaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
10 1007@pl00001930
Hochgeladen von
selvam123456789Copyright:
Verfügbare Formate
Journal of Orofacial Orthopedics
Fortschritte der Kieferorthopädie Original Article
Comparison of Modified Teuscher and Van Beek
Functional Appliance Therapies in High-Angle Cases
Vergleich der Therapie mit einer modifizierten
Teuscher-Apparatur und dem Funktionsgerät von
van Beek bei Fällen von ausgeprägtem vertikalen
Zahnwachstum
Neslihan Üçüncü1, Tamer Türk2, Carine Carels3
Abstract Zusammenfassung
The aim of this study was to investigate the effects of modified Ziel dieser Studie war, die skelettalen und dentoalveolären Aus-
Teuscher and van Beek functional appliances on the skeletal wirkungen einer Behandlung mit einer modifizierten Teuscher-
and dento-alveolar pattern in high-angle Class II, Division 1 Apparatur und der Therapie mit dem Funktionsgerät von van Beek
patients. bei 32 Klasse-II/1-Patienten mit ausgeprägtem vertikalen
The collective consisted of 32 patients with a high-angle Wachstumsmuster zu untersuchen.
Class II, Division 1 malocclusion. The modified Teuscher activa- Zwölf Patienten, im Durchschnitt 12 Jahre alt, erhielten den
tor was applied to a group of twelve patients, and the van Beek modifizierten Teuscher-Aktivator, eine weitere Gruppe von zehn
activator to a group of ten patients. A control group of ten sub- Patienten mit einem Durchschnittsalter von 11,8 Jahren wurde
jects was used for comparison purposes. The mean chrono- mit dem Van-Beek-Aktivator therapiert. Die Kontrollgruppe be-
logical ages of the groups were 12, 11.8 and 11.5 years, stand aus zehn Probanden, die im Durchschnitt 11,5 Jahre alt
respectively. 64 cephalograms taken before and after the treat- waren. 64 Fernröntgenbilder, die vor und nach der Behandlung
ment were evaluated. Intra-group measurement relations were angefertigt worden waren, wurden bewertet. Messwerte inner-
determined by the Wilcoxon test, and inter-group relations by halb einer Gruppe wurden mit Hilfe des Wilcoxon-Tests ausge-
analysis of variance and Duncan tests, using SPSS statistical wertet; zum Gruppenvergleich wurden die Varianzanalyse und der
software. Duncan-Test unter Benutzung der SPSS-Statistik-Software ange-
The following results were observed for both treated wandt.
groups without any change in growth direction: inhibition of Folgende Ergebnisse wurden bei beiden behandelten Grup-
maxillary growth, stimulation of mandibular growth, retrusion pen im Vergleich mit der Kontrollgruppe beobachtet, ohne dass
of upper incisors, distal tipping of upper molars, and reduction eine Änderung in der Wachstumsrichtung auftrat: Hemmung des
of overjet and overbite compared with the control group. The Wachstums der Maxilla, Anregung des Wachstums der Mandibula,
decrease in overbite in the van Beek group was due mainly to Retrusion der Oberkieferinzisivi, Distalkippung der Oberkiefermo-
intrusion of the incisors, and in the modified Teuscher group to laren, Reduktion von Frontzahnstufe und Überbiss. In der Van-
molar extrusion. Beek-Gruppe entstand die Reduktion des Überbisses im Wesentli-
Both activators were considered preferable in terms of ver- chen durch Intrusion der Inzisivi, in der mit der modifizierten
tical control of the facial height in high-angle cases with deep Teuscher-Apparatur behandelten Gruppe durch die Extrusion der
Molaren.
Beide Aktivatoren erwiesen sich zur vertikalen Kontrolle der
Gesichtshöhe bei Patienten mit ausgeprägt vertikalem Schä-
delaufbau und einem tiefen Überbiss als geeignet. Trotzdem war
1
Department of Orthodontics, Gazi University, Ankara, Turkey,
2
Department of Orthodontics, Ondokuz Mayis University, Samsun, Tur-
key,
3
Department of Orthodontics, Catholic University of Louvain,
Belgium. J Orofac Orthop/Fortschr Kieferorthop 2001;62:224–37
Received: March 28, 2000; accepted: June 15, 2000 DOI 10.1007/s00056-001-0020-2
224 J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel
Üçüncü N, et al. Vergleich von zwei Aktivator-Headgear-Therapieformen
overbite. However, stimulation of mandibular growth in the mo- die Stimulation des Unterkieferwachstums in der mit dem modi-
dified Teuscher activator group was found to be more signifi- fizierten Teuscher-Aktivator behandelten Gruppe signifikanter
cant than in the van Beek activator group. als in der Gruppe mit dem Van-Beek-Aktivator.
Key Words: Activator-headgear therapy · Van Beek activa- Schlüsselwörter: Aktivator-Headgear-Therapie ·
tor · Modified Teuscher activator · Skeletal Class II·Func- Van-Beek-Aktivator · Modifizierter Teuscher-Aktivator ·
tional treatment Skelettale Klasse II · Funktionskieferorthopädie
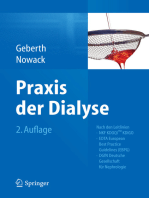
Figure 1b. Application of
modified Teuscher appliance.
Abbildung 1b. Modifizierte
Teuscher-Apparatur in situ.
Figure 1a. Modified Teuscher appliance.
Abbildung 1a. Modifizierte Teuscher-Apparatur.
Introduction Einleitung
The correction of Class II malocclusions with functional Die Korrektur von Klasse-II-Malokklusionen mittels Funk-
jaw orthopedics was first proposed by Andresen [2]. This tionskieferorthopädie wurde erstmals von Andresen [2]
approach was subsequently supported by numerous experi- vorgeschlagen. Später wurde dieser Ansatz durch zahlrei-
mental animal studies [12, 16]. che tierexperimentelle Studien unterstützt [12, 16].
Various researchers have asserted that activators reduce Verschiedene Untersucher haben bestätigt, dass Akti-
maxillary growth [4, 8, 9], stimulate mandibular growth [3, 4, vatoren das maxilläre Wachstum reduzieren [4, 8, 9], das
6, 9, 18] and induce mandibular backward rotations [8, 23]. mandibuläre Wachstum stimulieren [3, 4, 6, 9, 18] und außer-
Due to this rotational effect activators were contraindicated dem dorsal rotierte Unterkiefer nach anterior bringen [8,
in Class II high-angle cases, and activator-headgear combi- 23]. Aufgrund dieses Rotationseffekts waren Aktivatoren in
nations were developed for this purpose [3, 7, 18, 20, 21]. The Klasse-II-Fällen mit ausgeprägt vertikalem Schädelaufbau
use of combined activator-high pull headgear appliances has kontraindiziert. Deshalb wurden Aktivator-Headgear-Kom-
been recommended as a means of reducing vertical and sa- binationen entwickelt [3, 7, 18, 20, 21]. Die Benutzung von
gittal maxillary displacement, obtaining autorotations, and kombinierten Aktivator-Okzipitalheadgear-Apparaturen
increasing forward displacement of the mandible [17–19]. wurden als ein Hilfsmittel empfohlen, um die vertikale und
The activator developed by van Beek in 1982 has been re- sagittale Verschiebung der Maxilla zu reduzieren, eine Au-
ported to be effective in the reduction of overbite in deep torotation zu erhalten und die Ventralverschiebung der
bite and high-angle Class II cases [5, 21]. Mandibula zu fördern [17–19]. Der Aktivator, der von van
The aim of this study was to investigate the effects of the Beek im Jahr 1982 entwickelt wurde, erwies sich als effektiv
modified Teuscher and van Beek activators on the skeletal für die Bisshebung bei Klasse-II-Patienten mit Tiefbiss und
and dento-alveolar pattern in high-angle Class II, Division 1 ausgeprägtem vertikalen Wachstum [5, 21].
cases. Ziel dieser Studie war es, die skelettalen und dentoal-
veolären Auswirkungen des modifizierten Teuscher- und des
Patients and Methods Van-Beek-Aktivators bei Klasse-II/1-Fällen mit ausgepräg-
The 32 subjects enrolled in this study had an SN-MP angle tem vertikalen Wachstumsmuster zu untersuchen.
> 38º and a Class II, Division 1 malocclusion with severe
overjet and deep bite. A modified Teuscher activator (Fig- Patienten und Methode
ures 1a and 1b) was used in the first group comprising Die Studie umfasste 32 Patienten mit einem SN-MP-Win-
twelve patients with a mean chronological age of 12 years. kel von mehr als 38° und einer Klasse-II/1-Anomalie mit
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel 225
Üçüncü N, et al. Comparison of Two Activator-Headgear Therapies
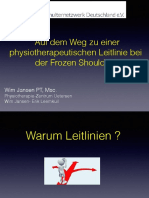
Figure 2b. Application of
Figure 2a. Van Beek appliance. van Beek appliance.
Abbildung 2a. Van-Beek-Apparatur. Abbildung 2b. Van-Beek-
Apparatur in situ.
A van Beek activator [21] (Figures 2a and 2b) was used in ausgeprägtem sagittalen und vertikalen Überbiss. Die erste
the second group consisting of ten patients with a mean Gruppe, die sich aus 12 Patienten im Alter von durch-
chronological age of 11.8 years. A group of ten untreated sub- schnittlich zwölf Jahren zusammensetzte, wurde mit dem
jects served as the control group. The patients comprising modifizierten Teuscher-Aktivator behandelt (Abbildungen
the treatment and control groups were matched according 1a und 1b). Bei der zweiten Gruppe, die aus zehn Patienten
to their sagittal and vertical growth patterns (Table 1). mit einem Durchschnittsalter von 11,8 Jahren bestand,
The modified Teuscher activator (MTA) group and the wurde ein Van-Beek-Aktivator [21] eingesetzt (Abbildun-
control group were selected from patients attending the De- gen 2a und 2b). Die Kontrollgruppe bestand aus zehn Pro-
partment of Orthodontics, Gazi University, Ankara, Turkey; banden. Die Patienten der Behandlungs- und der Kontroll-
the van Beek activator (VBA) group was selected from pa- gruppe wurden gemäß ihres sagittalen und vertikalen
tients registered with the Department of Orthodontics, Wachstumsmusters ausgewählt (Tabelle 1).
Catholic University of Louvain, Belgium. Die Gruppe mit modifiziertem Teuscher-Aktivator
Therapy groups were treated by one of the present (MTA) und die Kontrollgruppe wurde in der kieferorthopä-
authors at the respective department. The modified Teu- dischen Abteilung der Gazi-Universität, Ankara, Türkei, die
scher activator was designed according to the description Gruppe mit dem Van-Beek-Aktivator (VBA) wurde in der
given by Teuscher, but with a labial bow being used instead kieferorthopädischen Abteilung der katholischen Univer-
of torquing spurs. Stöckli & Teuscher [17] pointed out that sität Leuven, Belgien, ausgewählt.
“if torque control of the upper incisors is not critical, a stand- Die Behandlungsgruppen wurden innerhalb einer Ab-
ard labial wire (0.8 mm in diameter) with U-loops in the teilung von einem der Autoren behandelt. Der modifizierte
canine region may be used instead of torquing springs. The Teuscher-Aktivator wurde entsprechend der Beschreibung
acrylic extensions for the front teeth, however, should be the von Teuscher gestaltet, anstelle der Torquefedern wurde al-
same. With this setup a two-point contact situation is also lerdings ein Labialbogen benutzt. Stöckli & Teuscher [17]
Table 1. Comparison of ages and some cephalometric variables of the treatment groups and the control group at baseline.
Tabelle 1. Altersvergleich und kephalometrische Variablen der Behandlungs- und Kontrollgruppen zu Behandlungsbeginn.
Teuscher Van Beek Control p
Measurements Mean SD SE Mean SD SE Mean SD SE I–II II–III I–III
Chronological age 12.00 0.85 0.26 11.80 0.75 0.33 11.50 1.00 0.50 NS NS NS
ANB 6.33 1.09 0.36 6.00 1.44 0.25 5.42 0.53 0.43 NS NS NS
MP-SN 41.55 3.50 1.18 40.70 2.80 1.09 39.40 1.81 0.70 NS NS NS
Y-axis 73.27 3.51 1.17 71.42 3.69 1.39 72.50 3.25 1.22 NS NS NS
226 J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel
Üçüncü N, et al. Vergleich von zwei Aktivator-Headgear-Therapieformen
achieved that can provide some axial control of the upper gaben an, „wenn keine Torquekontolle der oberen Inzisivi
incisors, although to a much lesser degree than with torquing benötigt wird, kann ein gewöhnlicher Labialbogen (0,8 mm
auxiliaries.” Extra-oral force was 250–300 g per side and was Durchmesser) mit U-Schlaufen im Eckzahnbereich statt der
passed through the center of resistance of the maxilla. The Torquefedern benutzt werden. Die Kunststoffextensionen
thickness of the construction bite was approximately für die Frontzähne sollten jedoch beibehalten werden. Mit
4–5 mm. The labial bow was in contact with the maxillary diesem Aufbau kann auch ein Zwei-Punkt-Kontakt erreicht
incisors and free from the canines to allow for buccal werden, der eine Achsenkontrolle der oberen Inzisivi er-
expansion. Labial tipping of the mandibular incisors was möglicht, wenn auch zu einem geringeren Ausmaß als mit
limited by partially covering the labial surfaces with acrylic. den Torquefedern.“ Die extraoralen Kräfte betrugen
Trimming was not applied until the end of treatment. 250–300 g pro Seite und liefen durch das Widerstandszen-
The van Beek activator was constructed as described by trum der Maxilla. Die Dicke des Konstruktionsbisses betrug
van Beek [21]. The inner arms of the face-bow were in the in- ungefähr 4–5 mm. Der Labialbogen hatte Kontakt zu den
cisor region. The outer bows of the face-bow were directed oberen Schneidezähnen, nicht aber zu den Eckzähnen, um
approximately through the center of resistance of the maxil- eine Expansion in bukkaler Richtung zu ermöglichen. Eine
la. The magnitude of the extra-oral force was 300–350 g per Labialkippung der unteren Inzisiven wurde dadurch be-
side and the construction bite was 10 mm. The lower parts of grenzt, dass die Labialflächen zum Teil mit Kunststoff be-
the activator were not in contact with the lingual surfaces of deckt wurden. Bis zum Ende der Behandlung wurde nicht
the lower incisors, but the acrylic was extended beyond their eingeschliffen.
incisal edges. The upper parts covered the palatal half of the Der Van-Beek-Aktivator wurde nach den Angaben
occlusal surfaces of the premolars and molars, and the ante- von van Beek gestaltet [21]. Die inneren Arme des Ge-
rior teeth were enclosed in acrylic up to the cervical margin sichtsbogens befanden sich im Bereich der Schneidezähne.
for torque control. The occlusal surfaces of the upper molars Die Außenarme des Gesichtsbogens liefen ungefähr durch
and premolars were ground flat transversely, but the sagittal das Widerstandszentrum der Maxilla. Das Ausmaß der ex-
contour was left untrimmed. traoralen Kräfte betrug pro Seite 300–350 g, und der Kon-
In both appliances the extra-oral force direction is struktionsbiss hatte eine Stärke von 10 mm. Der untere Teil
backwards and upwards, and passes through the center of des Aktivators wies keinen Kontakt zu den Lingualflächen
resistance of the maxilla. In this way the vertical and sagit- der unteren Schneidezähne auf, der Kunststoff wurde je-
tal growth of the maxilla is inhibited. The force application doch bis über die Inzisalkanten extendiert. Der obere An-
point in the modified Teuscher activator is in the premolar teil bedeckte die palatinalen Hälften der Okklusalflächen
region (Figure 1a). However, the force application point in der Prämolaren und der Molaren, die Frontzähne wurden
the van Beek activator is more anterior, with the outer aufgrund der Torquekontolle bis zum zervikalen Rand in
bows of the extra-oral appliance being placed in the incisor Kunststoff eingebettet. Die okklusalen Flächen der oberen
region (Figure 2a). Therefore, these extra-oral forces, Molaren und Prämolaren wurden in transversaler Richtung
which have the same direction but a different line of action, plan eingeschliffen, die sagittalen Konturen wurden belas-
produce different outcomes. In the van Beek appliance, the sen.
exertion of intrusive force in the incisor region is more evi- Die Zugrichtung der extraoralen Kräfte war bei beiden
dent [17, 21]. Geräten nach hinten und oben und lief durch das Wider-
The patients were instructed to wear the activators for standszentrum der Maxilla. Auf diese Weise wird das verti-
12–14 hours per day. kale und sagittale Wachstum der Maxilla gehemmt. Der An-
In all cases the criterion for discontinuing active treat- griffspunkt der Kraft liegt beim modifizierten Teuscher-
ment was clinical reduction of the initial overbite and over- Aktivator in der Prämolarenregion (Abbildung 1a). Der
jet. The treatment period for both groups was 1 year on aver- Kraftangriffspunkt des Van-Beek-Aktivators liegt jedoch
age. weiter anterior, weil die Außenarme im Frontzahngebiet an-
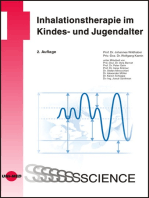
64 lateral cephalograms were obtained at the beginning gebracht sind (Abbildung 2a). Deshalb weisen diese extra-
and at the end of treatment. The cephalograms were traced oralen Kräfte, die dieselbe Richtung, aber einen anderen
and measured to the nearest 0.5 mm or 0.5º. Reference Ansatzpunkt haben, unterschiedliche Ergebnisse auf. Beim
lines – NSL (nasion sella line) and NSP (nasion sella perpen- Van-Beek-Aktivator ist die Wirkung der intrusiven Kräfte
dicular at sella) – were constructed. The linear and angular auf das Frontzahngebiet offensichtlicher [17, 21].
cephalometric measurements were based on these reference Die Patienten wurden angewiesen, die Aktivatoren
lines. The measurements are listed in Table 2 and shown in 12–14 Stunden am Tag zu tragen.
Figures 3 and 4. Das Kriterium für den Abbruch der aktiven Behand-
All radiographs were traced independently by one of lung war die klinische Reduktion des anfänglich vergrößer-
the authors. In order to check the cephalometric error of ten sagittalen und vertikalen Überbisses. Die Behandlungs-
method, 32 cephalograms were randomly selected from the dauer betrug bei beiden Gruppen im Durchschnitt 1 Jahr.
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel 227
Üçüncü N, et al. Comparison of Two Activator-Headgear Therapies
Table 2. Measurements evaluated.
Tabelle 2. Aufstellung der Messungen.
Maxillary and mandibular skeletal measurements
SNA Sella to nasion to point A angle
SNB Sella to nasion to point B angle
ANB Point A to nasion to point B angle
SN/PP Sella-nasion to palatal plane angle
Occ/SN Occlusal plane to sella-nasion angle
PP/MP Palatal plane to mandibular plane angle
SN/MP Sella-nasion to mandibular plane angle
Y-axis Sella-nasion to gnathion angle
S-Go Sella to gonion
N-Me Nasion to menton
Jar.Ratio Jarabak ratio (S-Go:N-Me)
N-ANS Nasion to anterior nasal spine Figure 3. Reference points and lines used for skeletal and dental
ANS-Me Anterior nasal spine to menton angular measurements.
Abbildung 3. Referenzpunkte und Linien für die skelettalen und
Upper dental measurements dentalen Winkelmessungen.
U1/SN Upper incisor axis to sella-nasion angle
U1-PP Distance from upper incisor tip to palatal plane
U6/SN Upper first molar crown angulations to sella-nasion angle
U6M-PP Distance from upper molar mesial tubercule to palatal plane
NSP⊥U1 Distance from upper incisor tip to nasion-sella perpendicular
line
NSP⊥U6D Distance from distal crown surface of upper first molar to
nasion-sella perpendicular line
Lower dental measurements
L1/MP Lower incisor axis to mandibular plane angle
MP-L1 Distance from lower incisor tip to mandibular plane
L6/MP Lower first molar crown angulations to mandibular plane
MP-L6M Distance from lower first molar’s mesial tubercule to
mandibular plane
NSP⊥L1 Distance from lower incisor tip to nasion-sella perpendicular
line
NSP⊥L6D Distance from distal crown surface of lower first molar to
nasion-sella perpendicular line
Interdental measurements
U6-L6 Intermolar crown distance on occlusal plane
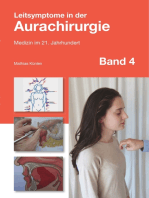
Figure 4. Reference points and lines used for skeletal and dental
Overjet Horizontal difference in upper and lower incisal edge position
linear measurements.
Overbite Vertical difference in upper and lower incisal edge position
Abbildung 4. Referenzpunkte und Linien für die skelettalen und den-
U1/L1 Interincisal angle
talen linearen Messungen.
228 J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel
Üçüncü N, et al. Vergleich von zwei Aktivator-Headgear-Therapieformen
Table 3. Reproducibility of measurements. Zu Beginn und zum Ende der Behandlung wurden 64
Tabelle 3. Reproduzierbarkeit der Messungen Fernröntgenseitenbilder angefertigt. Die Aufnahmen wur-
den durchgezeichnet und auf 0,5 mm bzw. 0,5° genau vermes-
sen. Als Referenzlinien wurden NSL (Nasion-Sella-Linie)
Measurements r Measurements r
und NSP (Senkrechte zu Nasion-Sella in Sella) konstruiert.
SNA 0.96 U6/SN 0.98 Die Abstandsmessungen und Winkel im Fernröntgenseiten-
SNB 0.98 U6M-PP 0.97
bild wurden in Bezug auf diese Referenzlinien durchgeführt.
Die Messungen sind in Tabelle 2 aufgeführt und in den Ab-
ANB 0.99 NSP⊥U1 0.97
bildungen 3 und 4 dargestellt.
SN-PP 0.95 NSP⊥U6D 0.98
Alle Röntgenbilder wurden unabhängig voneinander
Occ-SN 0.97 L1/MP 0.99
von einem der Autoren durchgezeichnet. Um den methodi-
PP-MP 0.96 MP-L1 0.99
schen Fehler der Fernröntgenseitenbildanalyse zu überprü-
SN-MP 0.98 L6/MP 0.98 fen, wurden 32 Fernröntgenseitenbilder zufällig aus den 64
Y-axis 0.97 MP-L6M 0.98 angefertigten ausgewählt, diese wurden 15 Tage später
S-Go 0.98 NSP⊥L1 0.99 nochmals von einem der Autoren durchgezeichnet und aus-
N-Me 0.99 NSP⊥L6D 0.97 gewertet. Der „Wiederholungskoeffizient“ für jede Variable
Jar.Ratio 0.97 U6-L6 0.97 wurde mit einer Varianzanalyse berechnet [22]. Tabelle 3
N-ANS 0.99 Overjet 0.99 gibt die Koeffizienten an (r = 0,97–0,99).
ANS-Me 0.98 Overbite 0.99 Die Abweichungen innerhalb der Gruppen wurden durch
U1/SN 0.99 U1/L1 0.98 den Wilcoxon-Test berechnet. Die Abweichungen zwischen
U1-PP 0.98 den Gruppen wurden mittels Varianzanalyse und dem Dun-
can-Test unter der Verwendung der SPSS-Software bestimmt.
Ergebnisse
Die Messungen und statistischen Auswertungen wurden in
zwei Gruppen eingeteilt: skelettale und dentale Verände-
rungen. Lineare Messungen wurden in Millimeter, Winkel
in Grad angegeben.
64 cephalograms used and were retraced and recalculated in-
dependently by one of the authors 15 days later. The “coeffi- Skelettale Veränderungen
cient of reproducibility” for each variable was calculated Die Beziehungen zwischen den Gruppen mit modifiziertem
from the analysis of variance [22]. The reproducibility values Teuscher-Aktivator und mit Van-Beek-Aktivator wiesen
are listed in Table 3 (r = 0.97– 0.99). eine beträchtliche Abnahme des SNA und ANB-Winkels,
Intra-group measurement changes were determined by eine Zunahme des SNB-Winkels sowie der Abstände S-Go,
the Wilcoxon statistical test. Measurement changes among N-Me und ANS-Me auf. In der Gruppe mit modifiziertem
the groups were determined by analysis of variance and Teuscher-Aktivator veränderten sich die Jarabak-Relation
Duncan tests, using SPSS statistical software. und der Abstand N-ANS beträchtlich. In der Gruppe mit
Van-Beek-Aktivator fanden sich keine bedeutenden Ver-
Results änderungen des Jarabak-Winkels und des Abstands N-
The measurements and statistical evaluations were divided ANS (Tabellen 4 und 5).
into two categories: skeletal changes and dental changes. Innerhalb der Kontrollgruppe konnten bedeutende
Linear measurements were given in millimeters and angu- Veränderungen nur bei den Messungen S-Go, Ne-Me und
lar measurements in degrees. N-ANS beobachtet werden (Tabelle 6).
Der Vergleich der Gruppen mit der Kontrollgruppe
Skeletal Changes wies eine Zunahme des SNB-Winkels und der Strecken S-
Inter-group relationships for the modified Teuscher activa- Go, N-Me und ANS-Me auf sowie eine Abnahme des ANB-
tor and van Beek activator groups showed a significant Winkels in der Gruppe mit modifiziertem Teuscher-Aktiva-
decrease in the SNA and ANB angles, and a significant in- tor. Andererseits kam es in der Gruppe mit Van-Beek-
crease in the SNB angle, S-Go, N-Me, and ANS-Me dimen- Aktivator zu einer Abnahme des ANB-Winkels, keinen Ver-
sions. The Jarabak ratio and the N-ANS dimension were änderungen des SNB-Winkels und der vertikalen Dimensio-
seen to change significantly in the modified Teuscher ac- nen im Vergleich zur Kontrollgruppe. Die skelettalen Verän-
tivator group. However, no significant changes in the Jara- derungen in der Gruppe mit modifiziertem Teuscher-Akti-
bak ratio and in the N-ANS dimension were observed in vator und mit Van-Beek-Aktivator unterschieden sich nicht,
the van Beek activator group (Tables 4 and 5). mit Ausnahme der S-Go-Strecke (Tabelle 7).
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel 229
Üçüncü N, et al. Comparison of Two Activator-Headgear Therapies
Table 4. Pre- and post-treatment measurement changes of the modified Teuscher activator group (n = 12) (*p < 0.05; **p < 0.01; ***p < 0.001).
Tabelle 4. Veränderungen der Messwerte vor und nach der Behandlung in der Gruppe mit modifiziertem Teuscher-Aktivator (n = 12) (*p < 0,05;
**p < 0,01; ***p < 0,001).
Beginning of treatment End of treatment
Measurements Mean SD Mean SD p
Maxillary and mandibular skeletal measurements
SNA 78.66 3.32 78.05 3.39 *
SNB 72.33 3.15 73.61 3.30 **
ANB 6.33 1.08 4.44 1.18 ***
SN-PP 10.05 2.80 10.66 2.33 –
Occ-SN 20.77 3.52 20.66 4.38 –
PP-MP 30.55 4.60 29.61 2.64 –
SN-MP 41.55 3.56 41.11 3.83 –
Y-axis 73.27 3.51 73.38 3.31 –
S-Go 70.22 3.96 74.88 3.14 ***
N-Me 121.88 4.19 126.88 2.75 ***
Jar.Ratio 57.60 2.63 58.92 1.83 *
N-ANS 54.05 2.25 55.61 2.58 ***
ANS-Me 67.88 3.42 71.33 4.20 ***
Upper dental measurements
U1/SN 100.88 5.15 96.00 5.45 *
U1-PP 33.50 2.95 32.88 2.48 –
U6/SN 66.00 6.89 62.77 6.75 *
U6M-PP 21.55 2.69 22.94 2.81 **
NSP⊥U1 59.50 6.77 56.92 7.48 **
NSP⊥U6D 22.33 5.36 21.44 6.05 –
Lower dental measurements
L1/MP 92.22 5.11 90.66 2.95 –
MP-L1 42.77 2.34 44.11 2.52 **
L6/MP 81.72 5.43 82.55 4.74 –
MP-L6M 30.33 3.27 33.05 2.87 **
NSP⊥L1 51.94 6.48 53.88 7.14 **
NSP⊥L6D 21.88 5.21 25.50 6.36 *
Interdental measurements
U6-L6 –0.55 2.03 5.00 2.15 ***
Overjet 8.11 2.32 3.22 1.00 ***
Overbite 6.22 2.59 3.22 1.90 **
U1/L1 125.33 5.76 132.66 4.44 **
Chronological 144.88 months 10.52 157.77 months 9.54 ***
age (12 years) (13.14 years)
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel
230
Üçüncü N, et al. Vergleich von zwei Aktivator-Headgear-Therapieformen
Table 5. Pre- and post-treatment measurement changes of the van Beek activator group (n = 10) (*p < 0.05; **p < 0.01).
Tabelle 5. Veränderungen der Messungen vor und nach der Behandlung in der Gruppe mit Van-Beek-Aktivator (n = 10) (*p < 0,05; **p < 0,01).
Beginning of treatment End of treatment
Measurements Mean SD Mean SD p
Maxillary and mandibular skeletal measurements
SNA 80.28 3.98 79.50 4.58 *
SNB 74.28 3.93 75.07 3.95 *
ANB 6.00 1.44 4.42 1.59 *
SN-PP 7.14 2.47 7.28 2.19 –
Occ-SN 18.00 3.26 17.85 3.43 –
PP-MP 33.00 1.00 33.42 1.36 –
SN-MP 40.71 2.88 41.50 2.53 –
Y-axis 71.42 3.69 71.92 4.10 –
S-Go 70.85 2.41 73.14 3.76 *
N-Me 119.57 5.70 123.57 6.19 **
Jar.Ratio 58.30 1.58 59.22 2.30 –
N-ANS 50.28 3.31 51.42 4.23 –
ANS-Me 69.57 2.57 72.14 2.67 **
Upper dental measurements
U1/SN 105.14 3.53 99.71 2.49 *
U1-PP 34.07 2.35 32.41 2.69 *
U6/SN 65.14 5.33 61.14 6.49 *
U6M-PP 22.14 1.81 22.64 2.28 –
NSP⊥U1 62.21 3.46 60.42 4.34 –
NSP⊥U6D 24.71 4.63 23.85 4.73 –
Lower dental measurements
L1/MP 93.14 5.08 93.14 7.55 –
MP-L1 43.85 1.86 45.64 1.2 *
L6/MP 80.85 3.97 79.42 2.29 –
MP-L6M 31.28 1.64 32.85 1.46 **
NSP⊥L1 57.00 4.51 58.07 5.19 –
NSP⊥L6D 27.10 5.39 29.35 5.69 *
Interdental measurements
U6-L6 1.07 1.39 4.28 1.86 **
Overjet 6.64 1.95 2.42 1.20 **
Overbite 6.21 1.28 2.78 1.34 **
U1/L1 121.00 6.60 125.00 6.55 *
Chronological 141.71 months 9.54 154.28 months 7.11 **
age (11.8 years) (12.85 years)
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel 231
Üçüncü N, et al. Comparison of Two Activator-Headgear Therapies
In the control group, significant changes were ob- Dentale Veränderungen
served only in the S-Go, Ne-Me and N-ANS measure- In der Gruppe mit modifiziertem Teuscher-Aktivator
ments (Table 6). waren die Palatinalkippung (U1/SN) und die Retrusion
The inter-group comparison showed an increase in the (NSP⊥U1) der oberen Inzisivi und Extrusion (U6M-PP)
SNB, S-Go, N-Me, ANS-Me dimensions, and a decrease in und Distalkippung (U6/SN) der oberen Molaren statistisch
the ANB angle for the modified Teuscher activator group signifikant (Tabelle 4). In der Gruppe mit Van-Beek-Akti-
compared with the control group. On the other hand, a vator waren die Palatinalkippung (U1/SN) und die Intru-
decrease in the ANB angle but no change in the SNB angle sion (U1-PP) der oberen Inzisivi und die Distalkippung der
and vertical facial dimension measurements was observed in oberen Molaren (U6/SN) statistisch signifikant (Tabelle 5).
the van Beek activator group compared with the control In der Kontrollgruppe traten Extrusion (U6M-PP) und
group. Skeletal changes between the modified Teuscher ac- leichte Mesialisierung (NSP⊥U6D) der oberen Molaren
tivator and the van Beek activator groups showed no diffe- und Extrusion der unteren Inzisivi (MP-L1) und Molaren
rences except for the S-Go dimension (Table 7). (MP-L6M) auf (Tabelle 6).
Die Gruppe mit modifiziertem Teuscher-Aktivator wies
Dental Changes eine Protrusion (NSP⊥L1) und Extrusion (MP-L1) der unte-
In the modified Teuscher activator group, palatoversion ren Inzisivi, Extrusion (MP-L6M) und Mesialisierung
(U1/SN) and retrusion (NSP⊥U1) of the upper incisors and (NSP⊥L6D) der unteren Molaren auf. In der Gruppe mit
extrusion (U6M-PP) and distal tipping (U6/SN) of the Van-Beek-Aktivator wurden dagegen eine Extrusion der
upper molars were found to be statistically significant unteren Inzisivi (MP-L1) und der Molaren (MP-L6M) und
(Table 4). In the van Beek activator group, palatoversion eine Mesialisierung der unteren Molaren (NSP⊥L6D) beob-
(U1/SN) and intrusion (U1-PP) of the upper incisors and achtet (Tabellen 4 und 5). In der Kontrollgruppe waren
distal tipping of the upper molars (U6/SN) were found to die Extrusion der unteren (MP-L6M) und oberen
be statistically significant (Table 5). Extrusion (U6M-PP) Molaren (U6M-PP), eine leichte Protrusion (NSP⊥L1) und
and slight mesialization (NSP⊥U6D) of the upper molars eine Extrusion (MP-L1) der unteren Inzisivi signifikant (Ta-
and extrusion of the lower incisors (MP-L1) and molars belle 6).
(MP-L6M) were recorded in the control group (Table 6). Im Vergleich mit der Kontrollgruppe wurden sowohl
Protrusion (NSP⊥L1) and extrusion (MP-L1) of the in der Gruppe mit modifiziertem Teuscher-Aktivator als
lower incisors and extrusion (MP-L6M) and mesialization auch in der mit Van-Beek-Aktivator eine Palatinalkippung
(NSP⊥L6D) of the lower molars were observed in the modi- (U1/SN), eine Retrusion (NSP⊥U1) der oberen Inzisivi und
fied Teuscher activator group, whereas extrusion of the eine Distalkippung der oberen Molaren festgestellt. Signifi-
lower incisors (MP-L1) and molars (MP-L6M) and mesial- kant waren in der Gruppe mit modifiziertem Teuscher-Akti-
ization of the lower molars (NSP⊥L6D) were observed in vator die Extrusion der unteren Molaren (MP-L6M) und in
the van Beek activator group (Tables 4 and 5). Extrusion of der mit Van-Beek-Aktivator die Intrusion der oberen Inzisi-
the lower (MP-L6M) and upper molars (U6M-PP), and vi im Vergleich mit der Kontrollgruppe (Tabelle 7).
slight protrusion (NSP⊥L1) and extrusion (MP-L1) of the
lower incisors were found to be significant in the control Veränderungen der Okklusion
group (Table 6). In beiden behandelten Gruppen wurden eine Abnahme
Inter-group comparison indicated palatoversion (U1/ des sagittalen und vertikalen Überbisses und eine Zu-
SN) and retrusion (NSP⊥U1) of the upper incisors and distal nahme des Interinzisalwinkels (U1/L1) sowie der Molaren-
tipping of the upper molars (U6/SN) for both the modified relation (U6-L6) aufgrund der korrigierten Klasse-II-Ok-
Teuscher activator and van Beek activator groups compared klusion beobachtet. Ein Vergleich der beiden behandelten
to the control group. In the modified Teuscher activator Gruppen wies keine signifikant unterschiedlichen Verände-
group, extrusion of the lower molars (MP-L6M), and in the rungen der Okklusion auf, abgesehen von der Molarenrela-
van Beek activator group intrusion of the upper incisors tion (Tabellen 4, 5 und 7).
(U1-PP) were found to be significant compared with the
control group (Table 7). Diskussion
Lange Zeit galt ein ausgeprägtes vertikales Wachstumsmus-
Interdental Changes ter als Kontraindikation für eine Aktivatortherapie. Später
A decrease in overjet and overbite and increases in the in- wurde jedoch festgestellt, dass mit einer Kombination von
terincisal angle (U1/L1) and in the U6-L6 dimension due to Aktivator mit Headgear gute Ergebnisse bei der Behand-
the corrected Class II occlusion were observed in both lung von Klasse-II-Fällen mit ausgeprägtem vertikalen
treated groups. Comparison of the interdental changes Wachstum zu erzielen sind.
between the treated groups showed no significant changes Diese Studie versucht die Auswirkungen zweier ver-
except for the U6-L6 measurement (Tables 4, 5 and 7). schiedener Aktivator-Headgear-Geräte bei Klasse-II-Fällen
232 J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel
Üçüncü N, et al. Vergleich von zwei Aktivator-Headgear-Therapieformen
Table 6. Pre- and post-treatment measurement changes of the control group (n = 10) (*p < 0.05; **p < 0.01).
Tabelle 6. Veränderungen der Messungen vor und nach der Behandlung in der Kontrollgruppe (n = 10) (*p < 0,05; **p < 0,01).
Beginning of control End of control
Measurements Mean SD Mean SD p
Maxillary and mandibular skeletal measurements
SNA 77.28 3.30 77.42 2.93 –
SNB 72.00 3.05 71.85 3.18 –
ANB 5.42 0.53 5.57 0.53 –
SN-PP 9.64 3.49 10.00 3.27 –
Occ-SN 22.57 4.23 22.71 3.25 –
PP-MP 30.14 3.23 29.00 3.10 –
SN-MP 39.42 1.81 40.00 2.14 –
Y-axis 72.50 3.25 72.64 3.35 –
S-Go 71.42 4.75 73.42 5.25 *
N-Me 117.00 5.03 119.42 5.22 *
Jar.Ratio 60.99 1.73 61.44 2.71 –
N-ANS 54.07 3.61 56.14 4.22 **
ANS-Me 66.42 3.69 67.71 3.8 –
Upper dental measurements
U1/SN 93.85 10.62 93.57 10.59 –
U1-PP 32.71 2.92 33.28 3.19 –
U6/SN 61.42 6.13 61.71 3.77 –
U6M-PP 20.14 2.54 21.28 2.49 *
NSP⊥U1 57.14 7.90 58.00 7.95 –
NSP⊥U6D 16.57 3.73 17.28 3.90 *
Lower dental measurements
L1/MP 90.00 5.50 92.00 5.32 –
MP-L1 39.92 1.30 41.07 1.69 *
L6/MP 87.14 3.28 88.00 4.72 –
MP-L6M 30.35 1.65 31.14 1.77 *
NSP⊥L1 50.14 6.03 51.5 6.18 *
NSP⊥L6D 14.00 4.20 15.28 4.18 **
Interdental measurements
U6-L6 0.28 1.25 0.14 2.03 –
Overjet 9.14 3.00 8.85 2.96 –
Overbite 3.71 1.79 3.71 1.79 –
U1/L1 126.71 8.44 126.42 8.03 –
Chronological 138.0 months 12.59 150.71 months 12.35 **
age (11.5 years) (12.6 years)
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel 233
Üçüncü N, et al. Comparison of Two Activator-Headgear Therapies
Table 7. Inter-group comparison of pre- and post-treatment differences (*p < 0.05).
Tabelle 7. Vergleich der Messungen vor und nach der Behandlung zwischen den Gruppen (*p < 0,05).
Modified Teuscher Van Beek Control p
Mean SD Mean SD Mean SD I–II II–III I–III
Measurements Maxillary and mandibular skeletal measurements
SNA –0.61 0.65 0.78 0.75 0.14 1.3 – – –
SNB 1.27 0.97 0.78 0.80 –0.15 1.2 – – *
ANB –1.88 1.05 –1.57 0.97 0.14 0.37 – * *
SN-PP 0.61 1.94 0.14 1.31 0.35 1.2 – – –
Occ-SN 0.11 2.26 0.14 2.60 0.14 1.46 – – –
PP-MP –0.94 2.62 0.42 0.73 –1.14 1.67 – – –
SN-MP –0.44 1.44 0.78 0.78 0.57 0.57 – – –
y-axis 0.11 1.02 0.50 1.04 0.14 0.89 – – –
S-Go 4.66 2.50 2.29 1.80 2.00 1.41 * – *
N-Me 5.05 2.94 4.00 1.53 2.42 1.60 – – *
Jar.Ratio 1.31 1.83 –0.08 1.42 0.45 1.34 – – –
N-ANS 1.53 1.27 1.14 1.44 2.07 1.10 – – –
ANS-Me 3.45 2.69 2.57 0.79 1.29 1.38 – – *
Upper dental measurements
U1/SN –4.88 5.08 –5.42 4.50 –0.28 1.62 – * *
U1-PP –0.61 1.11 –1.66 1.44 0.57 0.78 – * –
U6/SN –3.22 3.19 –4.00 3.05 0.28 4.78 – * *
U6M-PP 1.39 0.50 0.50 0.96 1.14 0.90 – – –
NSP⊥U1 –2.57 2.14 –1.78 3.05 0.85 0.89 – * *
NSP⊥U6D –0.88 1.93 –0.85 1.62 –0.71 0.48 – – –
Lower dental measurements
L1/MP –1.55 4.00 0.00 3.51 2.00 1.63 – – –
MP-L1 1.33 1.08 1.78 1.14 1.14 0.89 – – –
L6/MP 0.83 2.57 –1.42 3.50 0.85 3.02 – – –
MP-L6M 2.72 1.92 1.57 0.53 0.79 0.70 – – *
NSP⊥L1 1.94 1.82 1.07 1.51 1.35 0.49 – – –
NSP⊥L6D 3.61 2.20 2.25 3.77 1.28 0.69 – * *
Interdental measurements
U6-L6 5.05 1.50 3.21 1.03 0.14 1.34 * * *
Overjet –4.88 1.85 –4.21 1.72 –0.28 1.11 – * *
Overbite –3.00 1.47 –3.42 1.53 0.42 0.97 – * *
U1/L1 7.33 6.72 4.00 3.69 –0.28 3.09 – – *
Treatment 12.9 3.98 12.5 4.69 12.7 4.72 – – –
time months months months
234 J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel
Üçüncü N, et al. Vergleich von zwei Aktivator-Headgear-Therapieformen
Discussion mit vertikalem Wachstumsmuster zu beurteilen. Die inneren
High-angle cases had long been regarded as a contraindica- Arme des Gesichtsbogens wurden in der Gruppe mit modi-
tion for the use of activators. However, the combination of fiziertem Teuscher-Aktivator in der Prämolarenregion ange-
activator and headgear appliances subsequently showed ef- bracht, in der mit Van-Beek-Aktivator hingegen im Schnei-
fective outcomes in the treatment of high-angle Class II dezahnbereich, was sich als vorteilhafter für die Bisshebung
cases. herausstellte [5, 21]. Zur Bewertung der Auswirkungen die-
This clinical study was aimed at evaluating the effects of ser Aktivatoren wurde eine Kontrollgruppe gebildet, die das
two different activator-headgear appliances in high-angle gleiche Wachstumsmuster aufwies.
Class II cases. In the modified Teuscher activator group, the Dermaut et al. [5] beobachteten einen geringen Wachs-
application of the inner arms of the face-bow was in the pre- tumsreiz auf den Unterkiefer und keine Hemmung des
molar region, whereas in the van Beek activator group the Oberkieferwachstums bei mit Van-Beek-Aktivator behan-
inner bow application was displaced anteriorly, in the incisor delten Patienten. Ngan et al. [13] stellten eine Verringerung
region. The van Beek activator design has been shown to be des anterioren Wachstums der Maxilla fest, fanden aber kei-
advantageous for the opening of deep bites [5, 21]. For ne signifikanten Veränderungen in Bezug auf die Unterkie-
evaluation of the effects of these activators, a control group fervorverlagerung. Bei den behandelten Gruppen dieser
demonstrating the same growth pattern was set up. Studie zeigte sich nur eine geringe Hemmung des maxillären
Dermaut et al [5] observed minor growth stimulations of Wachstums (Tabellen 4 und 5), im Vergleich mit der Kon-
the mandible and no inhibition of maxillary growth in the trollgruppe konnten aber keine statistisch signifikanten Ver-
van Beek activator group. Ngan et al [13] found a reduction änderungen beobachtet werden (Tabelle 7).
of the forward growth of the maxilla but no significant Einige Untersucher berichteten, dass Aktivatoren das
changes in the forward mandibular displacements. In the Wachstum der Mandibula nach anterior fördern [3, 9, 15, 18].
treatment groups of the present study, there was little reduc- In dieser Studie war die Ventralbewegung der Mandibula in
tion of maxillary growth (Tables 4 and 5); compared to the der Gruppe mit modifiziertem Teuscher-Aktivator und in
control group, no statistically significant changes were ob- der mit Van-Beek-Aktivator signifikant (Tabellen 4 und 5),
served (Table 7). aber es gab keine signifikante Stimulation des Unterkiefer-
Some investigators have reported that activators pro- wachstums, wenn man die Gruppe mit Van-Beek-Aktivator
mote forward growth of the mandible [3, 9, 15, 18]. In the mit der Kontrollgruppe verglich (Tabelle 7).
present study, the forward movement of the mandible was Levin [11] postulierte, dass eine kombinierte Aktivator-
significant in the modified Teuscher activator and van Beek Headgear-Behandlung bei dolichofazialem Gesichtsschä-
activator groups (Tables 4 and 5), but there was no signifi- delaufbau eine Rotation des Unterkiefers im Uhrzeigersinn
cant stimulation of the mandible in the van Beek activator hervorrufen könnte. Nielson & Lagerström [14] berichteten,
group compared with the control group (Table 7). dass sie bei 40 Patienten Headgear-Aktivatoren im Zuge der
Levin [11] stated that combined activator-headgear Behandlung einsetzten und fanden, dass bei einigen dieser
treatment might induce clockwise mandibular rotations in 40 Patienten eine posteriore oder anteriore Rotation der
dolichofacial types. Nielsen & Lagerström [14] reported that Mandibula auftrat. Dennoch wurde festgestellt, dass die re-
they applied activator-headgear to 40 patients and indicated sultierenden Rotationen statistisch nicht signifikant waren.
that posterior mandibular rotation or anterior mandibular In unserer Studie ergab sich für die Mandibularebene keine
rotation was observed in some of the 40 patients. However, signifikante Veränderung (Tabelle 7), obwohl die anteriore
the resulting rotations were found to be statistically insignifi- und posteriore Gesichtshöhe (S-Go, N-Me) bei beiden Be-
cant. In our study, although the anterior and posterior facial handlungsgruppen im Vergleich mit der Kontrollgruppe ei-
heights (S-Go, N-Me) showed a significant increase (Tables 4 nen signifikanten Anstieg zeigten (Tabellen 4 und 5).
and 5) in both treatment groups compared with the control Während eine Zunahme der unteren Gesichtshöhe in bei-
group, the mandibular plane angle demonstrated no significant den Gruppen beobachtet wurde, war der Zuwachs in der
change (Table 7). Whilst an increase of lower facial height was Gruppe mit modifiziertem Teuscher-Aktivator stärker aus-
observed in both groups, it was more pronounced in the mo- geprägt als in der Kontrollgruppe. Einige Untersucher be-
dified Teuscher activator group than in the control group. richteten, dass durch eine kombinierte Aktivator-Headgear-
Several researchers reported that combined activator-head- Therapie die untere Gesichtshöhe signifikant zunahm [7, 11,
gear treatment resulted in a significant increase in lower facial 13]. Das stimmt mit den Resultaten unserer Studie überein.
height [7, 11, 13,]. This is in line with the results of our study. In den behandelten Gruppen konnte eine deutliche Ab-
In the treatment groups a significant decrease in the nahme des ANB-Winkels (Tabellen 4 und 5) beobachtet
ANB angle was observed (Tables 4 and 5); however, no diffe- werden, es konnte jedoch kein Unterschied zwischen den
rence was observed between the treatment groups (Table 7). Gruppen festgestellt werden (Tabelle 7).
Although the van Beek activator group had total acrylic Obwohl die Gruppe mit Van-Beek-Aktivator eine voll-
coverage for torque control, both groups demonstrated pala- ständige Kunststoffüberkappung zur Torquekontrolle hatte,
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel 235
Üçüncü N, et al. Comparison of Two Activator-Headgear Therapies
toversion and retrusion of the upper incisors (Tables 4 and zeigten beide Gruppen eine Palatinalkippung und Retrusion
5). However, Aelbers & Dermaut [1] reported that a better der oberen Schneidezähne (Tabellen 4 und 5). In der Studie
torque control of the upper incisors was obtained with a von Aelbers & Dermaut [1] hingegen konnte mit einem ein-
simple modified Teuscher activator. fach modifizierten Teuscher-Aktivator eine bessere Torque-
Lagerström et al [10] reported that Class II correction kontrolle der oberen Schneidezähne erreicht werden.
was often achieved by distal repositioning of the maxillary Lagerström et al. [10] berichteten, dass die Korrektur
teeth and mesial repositioning of the mandibular teeth. In der Klasse II häufig durch Distalisierung der Oberkieferzäh-
both treatment groups distal tipping of the upper molars to ne und Mesialisierung der Unterkieferzähne erfolgt. In bei-
the SN plane was observed, whereas the lower molars den Behandlungsgruppen konnte eine Distalkippung der
showed extrusion (Tables 4 and 5). The measurement oberen Molaren zur SN-Ebene beobachtet werden. Im Ge-
changes between the molars (U6-L6) showed a significant gensatz dazu extrudierten die unteren Molaren (Tabellen 4
increase due to the Class I molar relationship obtained; this und 5). Die Messveränderungen der Molarenrelation (U6-
increase was more pronounced in the modified Teuscher L6) zeigten eine deutliche Zunahme aufgrund der erreichten
activator group (Table 7). Klasse-I-Situation; dies war ausgeprägter in der Gruppe mit
In the modified Teuscher activator group, the overjet modifiziertem Teuscher-Aktivator (Tabelle 7).
was decreased by the palatal tipping and retrusion of the up- In der Gruppe mit modifiziertem Teuscher-Aktivator
per incisors and the forward growth of the mandible (Table reduzierte sich die sagittale Frontzahnstufe durch die Pala-
4). In the van Beek activator group, the overjet was tinalkippung und Retrusion der Oberkieferschneidezähne
decreased by the palatal tipping and retrusion of the upper und das Vorwärtswachstum des Unterkiefers (Tabelle 5).
incisors and by only minor forward growth of the mandible Eine signifikante Verringerung des vertikalen Überbisses
(Table 5). A significant reduction in overbite was observed in wurde in beiden Gruppen beobachtet. Die Reduktion des
both groups. In the van Beek activator group this reduction Überbisses in der Gruppe mit Van-Beek-Aktivator kann im
can be attributed to the 1.66 mm intrusion of the incisors and Zusammenhang mit der Intrusion der Schneidezähne von
not to extrusion of the lower molars (Tables 5 and 7). How- 1,66 mm stehen und nicht mit der Extrusion der unteren
ever, in the modified Teuscher activator group it was due Molaren (Tabellen 5 und 7). In der Gruppe mit modifizier-
mainly to extrusion of the lower molars and not to intrusion tem Teuscher-Aktivator dagegen lässt sich die Reduktion
of the upper incisors (Tables 4 and 7). des Überbisses hauptsächlich auf die Extrusion der unteren
Dermaut et al [5] observed the same changes for the und nicht auf die Intrusion der oberen Frontzähne zurück-
overjet and overbite variables in the van Beek activator führen (Tabellen 4 und 7).
group. Dermaut et al. [5] konnten die gleichen Veränderungen
für den sagittalen und vertikalen Überbiss bei Patienten mit
Conclusions Van-Beek-Aktivator beobachten.
1. Without any change in growth direction, the following
results were observed for both treatment groups compared Schlussfolgerungen
with the control group: reduction of the ANB angle, 1. Ohne Veränderung der Wachstumsrichtung wurden
retrusion and palatoversion of the upper incisors, distal tip- die folgenden Ergebnisse für beide Behandlungsgruppen im
ping of the upper molars, and reduction of overjet and over- Vergleich mit der Kontrollgruppe festgestellt: Verringerung
bite. des ANB-Winkels, Retrusion und Palatinalkippung der obe-
2. Without any significant increase in lower facial height, ren Inzisivi, Distalkippung der oberen Molaren und Reduk-
a reduction of overbite was obtained when the van Beek tion des sagittalen und vertikalen Überbisses.
activator appliance was used in deep-bite and high-angle 2. Eine Reduktion des Überbisses wurde ohne signifi-
Class II, Division 1 cases. This reduction is considered to kante Zunahme der unteren Gesichtshöhe erreicht, wenn
result from intrusion of the upper incisors. Both appliances die Van-Beek-Apparatur bei Tiefbiss und Klasse II/1 mit
can be successfully used in deep-bite and high-angle Class II, ausgeprägtem vertikalen Wachstumsmuster eingesetzt wur-
Division 1 cases. However, in cases with prominent upper de. Diese Reduktion des Überbisses ist die Folge der Intrusi-
incisors the van Beek activator is more favorable. on der oberen Frontzähne. Beide Apparaturen können er-
3. Stimulation of mandibular growth in the modified folgreich bei Tiefbiss und Klasse II/1 mit ausgeprägtem ver-
Teuscher activator group was found to be more significant tikalen Wachstumsmuster verwendet werden, in Fällen mit
than in the van Beek activator group compared with the con- prominent erscheinenden oberen Schneidezähnen ist die
trol group. Apparatur von van Beek zu bevorzugen.
3. Die Stimulation des Unterkieferwachstums war in der
Acknowledgments Gruppe mit modifiziertem Teuscher-Aktivator signifikant
The authors would like to thank Professor Carine Carels for pro- höher als in der mit Van-Beek-Aktivator verglichen mit der
viding the data of the van Beek group. Kontrollgruppe.
236 J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel
Üçüncü N, et al. Vergleich von zwei Aktivator-Headgear-Therapieformen
References Danksagung
1. Aelbers CMF, Dermaut L. Incisor torque by means of a modified Teu- Die Autoren danken Prof. Carine Carels für die Bereitstellung der
scher activator (three case reports). J Orofac Orthop/Fortschr Kie- verwendeten Daten der Van-Beek-Gruppe.
ferorthop 1998;59:171–7.
2. Andresen V. The Norwegian system of functional gnatho-orthope-
dics. Acta Gnathol 1936;1:5–36.
3. Bass NM. Dento-facial orthopedics in the correction of the Class II
malocclusion. Br J Orthod 1982;9:3–31. Correspondence Address
4. Demisch A. Effects of activator therapy on the craniofacial skeleton Assoc. Prof. Dr. Neslihan Üçüncü
in Class II, division 1 malocclusion. Trans Eur Orthod Soc 1972; Gazi University
295–309. Department of Orthodontics
5. Dermaut LR, van den Eynde F, de Pauw G. Skeletal and dento-alveo- Faculty of Dentistry
lar changes as a result of headgear activator therapy related to dif-
06510 Emek Ankara
ferent vertical growth patterns. Eur J Orthod 1992; 14:140–6.
Turkey
6. Gürsoy S. Ortopedik fonksiyonel tedavi sonucu maksilla, mandibula
ve articulatio temporo mandibularis’te meydana gelen degisiklikle- Phone (+90/312) 215-3350, Fax -5199,
rin sefalometrik tetkiki. Istanbul University: Doctoral Thesis, 1968. e-mail: murat.ucuncu@tr.net or
7. Hansson C, Sköld B, Linder-Aronson S. Treatment of adolescents ucuncu@tr.net
with Hansaplate/Headgear. J Orofac Orthop/Fortschr Kieferorthop
1997;58:16–29.
8. Harvold EP, Vargervik K. Morphogenetic response to activator treat-
ment. Am J Orthod 1971;60:478–90.
9. Jacobsson SO. Cephalometric evaluation of treatment effect on
Class II, division 1 malocclusions. Am J Orthod 1967;53:446–55.
10. Lagerström LO, Nielsen L, Lee R, et al. Dental and skeletal contri-
butions to occlusal correction in patients treated with the high-pull
headgear-activator combination. Am J Orthod Dentofacial Orthop
1990;97:495–504.
11. Levin RI. Activator headgear therapy. Am J Orthod 1985;87:
91–109.
12. McNamara JA Jr. Neuromuscular and skeletal adaptations to altered
function in the orofacial region. Am J Orthod 1973; 64:548–606.
13. Ngan P, Wilson S, Florman M, et al. Treatment of Class II openbite
in the mixed dentition with a removable functional appliance and
headgear. Quintessenz Int 1992;23:323–33.
14. Nielsen IL, Lagerström LO. Individuelle Reaktion auf die Behand-
lung mit dem Headgear-Aktivator nach Teuscher. Inform Orthod
Kieferorthop 1993;3:303–22.
15. Pfeiffer JP, Grobéty D. A philosophy of combined orthopedic-ortho-
dontic treatment. Am J Orthod 1982;81:185–201.
16. Stöckli PW, Willert HG. Tissue reactions in the temporomandibular
joint resulting from anterior displacement of the mandible in the
monkey. Am J Orthod 1971;60:142–55.
17. Stöckli PW, Teuscher UM. Combined activator headgear orthope-
dics. In: Graber TM, Vanarsdall RL Jr, eds. Orthodontics: current
principles and techniques. St. Louis: Mosby, 1994:437–506.
18. Teuscher UM. A growth-related concept for skeletal Class II
treatment. Am J Orthod 1978;74:258–75.
19. Teuscher UM. An appraisal of growth and reaction to extraoral
anchorage. Simulation of orthodontic-orthopedic results. Am J
Orthod 1986;89:113–21.
20. Thurow RC. Craniomaxillary orthopedic correction with en masse
dental control. Am J Orthod 1975;68:601–24.
21. van Beek H. Overjet correction by a combined headgear and ac-
tivator. Eur J Orthod 1982;4:279–90.
22. Winner BJ. Statistical principles in experimental design, 2nd edn.
New York: McGraw-Hill, 1971.
23. Woodside DG. Some effects of activator treatment on the mandible
and the midface. Trans Eur Orthod Soc 1973;443–7.
J Orofac Orthop/Fortschr Kieferorthop 2001 · No. 3 © Urban & Vogel 237
Das könnte Ihnen auch gefallen
- Beneslider JOOFDokument14 SeitenBeneslider JOOFHeni KallosNoch keine Bewertungen
- Das HUNEKE Phänomen - Eine Patienteninformation über Klassische Neuraltherapie nach Dr. HUNEKEVon EverandDas HUNEKE Phänomen - Eine Patienteninformation über Klassische Neuraltherapie nach Dr. HUNEKENoch keine Bewertungen
- EWC SistemDokument14 SeitenEWC SistemRümeysa AydınNoch keine Bewertungen
- Lehnen2011.pdf Tad PainDokument10 SeitenLehnen2011.pdf Tad PainSuli M ENoch keine Bewertungen
- Sinergetische Reflextherapie Der Spastischen Beine...Dokument10 SeitenSinergetische Reflextherapie Der Spastischen Beine...seleditNoch keine Bewertungen
- Minitornillo en Cresta Ziiigoomatica en Paciente en CrecimientoDokument12 SeitenMinitornillo en Cresta Ziiigoomatica en Paciente en CrecimientoBraulio CaroNoch keine Bewertungen
- Die Unterkieferverlagerung Nach Obwegeserdal Pont Aus PatientensichtDokument4 SeitenDie Unterkieferverlagerung Nach Obwegeserdal Pont Aus PatientensichtWolle HartzNoch keine Bewertungen
- Palma Mini SlingDokument7 SeitenPalma Mini SlingrafaelmmoroniNoch keine Bewertungen
- Handrehabilitation: Für Ergotherapeuten und Physiotherapeuten, Band 3: Manuelle Therapie, Physikalische Maßnahmen, SchienenVon EverandHandrehabilitation: Für Ergotherapeuten und Physiotherapeuten, Band 3: Manuelle Therapie, Physikalische Maßnahmen, SchienenBirgitta Waldner-NilssonNoch keine Bewertungen
- Myofasziale Schmerzen und Funktionsstörungen: Diagnostik und TherapieVon EverandMyofasziale Schmerzen und Funktionsstörungen: Diagnostik und TherapieNoch keine Bewertungen
- FBL Klein-Vogelbach Functional Kinetics BehandlungstechnikenVon EverandFBL Klein-Vogelbach Functional Kinetics BehandlungstechnikenNoch keine Bewertungen
- AtemtherapeutischerDokument6 SeitenAtemtherapeutischermihaela.ostroveanu94Noch keine Bewertungen
- Leitsymptome in der Aurachirurgie Band 10: Medizin im 21. JahrhundertVon EverandLeitsymptome in der Aurachirurgie Band 10: Medizin im 21. JahrhundertNoch keine Bewertungen
- 1x1 der ambulanten Chirurgie: Qualitätsstandards und WirtschaftlichkeitVon Everand1x1 der ambulanten Chirurgie: Qualitätsstandards und WirtschaftlichkeitNoch keine Bewertungen
- 1 x 1 der ambulanten Chirurgie: Qualitätsstandards und WirtschaftlichkeitVon Everand1 x 1 der ambulanten Chirurgie: Qualitätsstandards und WirtschaftlichkeitNoch keine Bewertungen
- Komplikationsmanagement nach Stimmrehabilitation mit StimmprothesenVon EverandKomplikationsmanagement nach Stimmrehabilitation mit StimmprothesenNoch keine Bewertungen
- KontrakturenprophylaxeDokument22 SeitenKontrakturenprophylaxeLoys Park100% (2)
- Unifiziertes Vertebrologisch-Schmerztherapeutisches KonzeptVon EverandUnifiziertes Vertebrologisch-Schmerztherapeutisches KonzeptNoch keine Bewertungen
- Altintas 2016Dokument8 SeitenAltintas 2016Dr Ahmed NabilNoch keine Bewertungen
- Faszientherapie mit dem KLINEA-Konzept: Eine gelenkschonende Methode für Therapeut und PatientVon EverandFaszientherapie mit dem KLINEA-Konzept: Eine gelenkschonende Methode für Therapeut und PatientNoch keine Bewertungen
- Restoration of Lost Vertical Dimension With Cad CamDokument14 SeitenRestoration of Lost Vertical Dimension With Cad CamdentureNoch keine Bewertungen
- Leitsymptome in der Aurachirurgie Band 11: Medizin im 21. JahrhundertVon EverandLeitsymptome in der Aurachirurgie Band 11: Medizin im 21. JahrhundertNoch keine Bewertungen
- Complications in OVHDokument6 SeitenComplications in OVHFiorella YavarNoch keine Bewertungen
- Peat PDFDokument49 SeitenPeat PDFScribdTranslationsNoch keine Bewertungen
- Bourauel 2000Dokument14 SeitenBourauel 2000lauNoch keine Bewertungen
- 249 CMF 15 03 Greven SCREEN-mWMDokument12 Seiten249 CMF 15 03 Greven SCREEN-mWMСаша АптреевNoch keine Bewertungen
- Pflegeplan Für CellulitisDokument7 SeitenPflegeplan Für CellulitisScribdTranslationsNoch keine Bewertungen
- Flyer Interventionelle Schmerztherapie CT PDFDokument3 SeitenFlyer Interventionelle Schmerztherapie CT PDFtomili85Noch keine Bewertungen
- Wörterliste PflegekraefteDokument8 SeitenWörterliste PflegekraefteNeda KaranovicNoch keine Bewertungen
- Comparative Clinical Efficacy and Tolerability of Oxerutins and - HorseDokument5 SeitenComparative Clinical Efficacy and Tolerability of Oxerutins and - HorseRosa CarrilloNoch keine Bewertungen
- Maximum Anchorage in Orthodontics PDFDokument12 SeitenMaximum Anchorage in Orthodontics PDFSoe San KyawNoch keine Bewertungen
- Videofeedback Fentes PalatinesDokument5 SeitenVideofeedback Fentes PalatinesEtienneNoch keine Bewertungen
- Für Chirurgie Der KleintiereDokument5 SeitenFür Chirurgie Der KleintiereGER4SOULNoch keine Bewertungen
- Undlagen Des Bobath-Konzeptes Gabi Jacobs Und Renate Kohl Pflegezeitschrift Jg.65 Heft 1Dokument4 SeitenUndlagen Des Bobath-Konzeptes Gabi Jacobs Und Renate Kohl Pflegezeitschrift Jg.65 Heft 1Миодраг ЈовановићNoch keine Bewertungen
- Eberhardt 2019Dokument7 SeitenEberhardt 2019christian roblesNoch keine Bewertungen
- Prof. Uhlemann Artikel Heilfasten Bei ArthroseDokument8 SeitenProf. Uhlemann Artikel Heilfasten Bei ArthroseWartungNoch keine Bewertungen
- Folder Flap PalatoplastyDokument8 SeitenFolder Flap PalatoplastyvetermanNoch keine Bewertungen
- Behandlungsstandards PhysiotherapieDokument42 SeitenBehandlungsstandards Physiotherapiegiovanoti100% (2)
- Mucocele On The Lower Lip - A Case Report PDFDokument3 SeitenMucocele On The Lower Lip - A Case Report PDFpaolaNoch keine Bewertungen
- Arzt Dsh-PruefungsmusterlvDokument14 SeitenArzt Dsh-PruefungsmusterlvSzarka GabriellaNoch keine Bewertungen
- 7 Untersuchung Des FussesDokument35 Seiten7 Untersuchung Des FussesCorrado BertottoNoch keine Bewertungen
- 086 ZaehneDokument3 Seiten086 ZaehneindrielaNoch keine Bewertungen
- MORCELADORDokument8 SeitenMORCELADORDante MelendezNoch keine Bewertungen
- Retrospective Clinical Investigation of The ImpacDokument9 SeitenRetrospective Clinical Investigation of The ImpacSusana CalleNoch keine Bewertungen
- Frozen ShoulderDokument49 SeitenFrozen ShoulderQuynh Anh NguyenNoch keine Bewertungen
- SOP Hammer ReflekDokument2 SeitenSOP Hammer ReflekRaihan PutraNoch keine Bewertungen
- Original Article: Journal of Orofacial Orthopedics Fortschritte Der KieferorthopädieDokument14 SeitenOriginal Article: Journal of Orofacial Orthopedics Fortschritte Der KieferorthopädieClaudiaNoch keine Bewertungen
- CMF - 2019 - Planesystem1 2Dokument24 SeitenCMF - 2019 - Planesystem1 2Fernando Ari del CorroNoch keine Bewertungen
- Interaktive Telemedizinische Betreuung Von Beatmungspatienten. Eindrücke Vom Modellvorhaben EViVaDokument24 SeitenInteraktive Telemedizinische Betreuung Von Beatmungspatienten. Eindrücke Vom Modellvorhaben EViVaw.moellerNoch keine Bewertungen
- Dissertation FSDokument93 SeitenDissertation FSRamadhan Yudha PratamaNoch keine Bewertungen
- Leitsymptome in der Aurachirurgie Band 4: Medizin im 21. JahrhundertVon EverandLeitsymptome in der Aurachirurgie Band 4: Medizin im 21. JahrhundertNoch keine Bewertungen
- Physiotherapie Anlage 5 Zulassungsvoraussetzungen BFDokument6 SeitenPhysiotherapie Anlage 5 Zulassungsvoraussetzungen BFGreatNoch keine Bewertungen
- DZA 3 2016 Innovation Zeise-SuessDokument4 SeitenDZA 3 2016 Innovation Zeise-SuessJessica Pérez PérezNoch keine Bewertungen